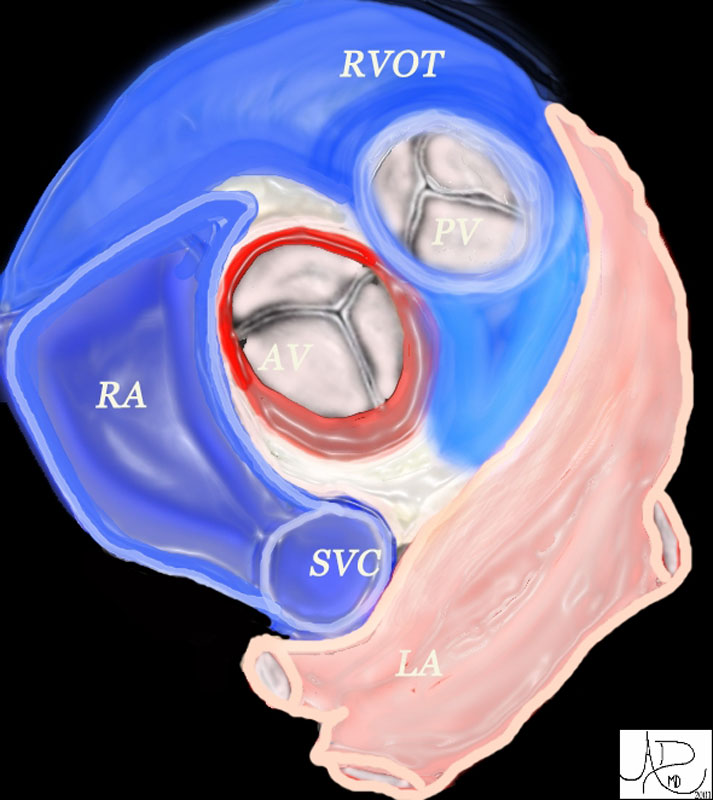
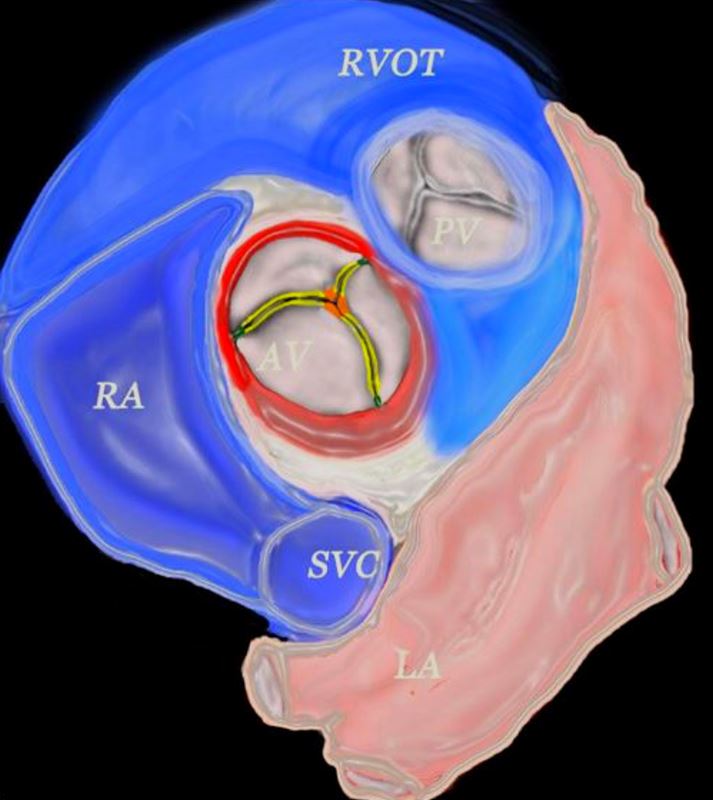
The Aortic Annulus (red ring) and Aortic Valve 47681 heart cardiac aortic valve aorta right atrium right atrial appendage left atrial appendage LAA RAA pulmonary valve right ventricular outflow tract left atrium LA RA RVOT anatomy normal position relations Ashley Davidoff
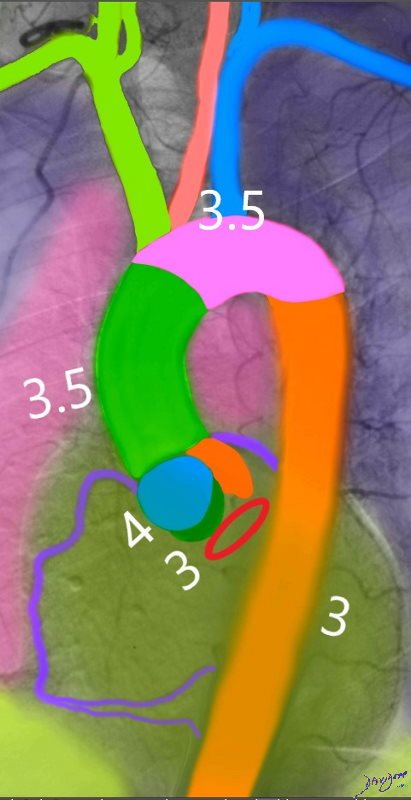
Upper Limits Diameters of the Aorta Ashley Davidoff Upper limits of the functional annulus consisting of the fibrous base ((bright red) sinuses and leaflets (maroon) and sinotubular junction (white) Ashley Davidoff
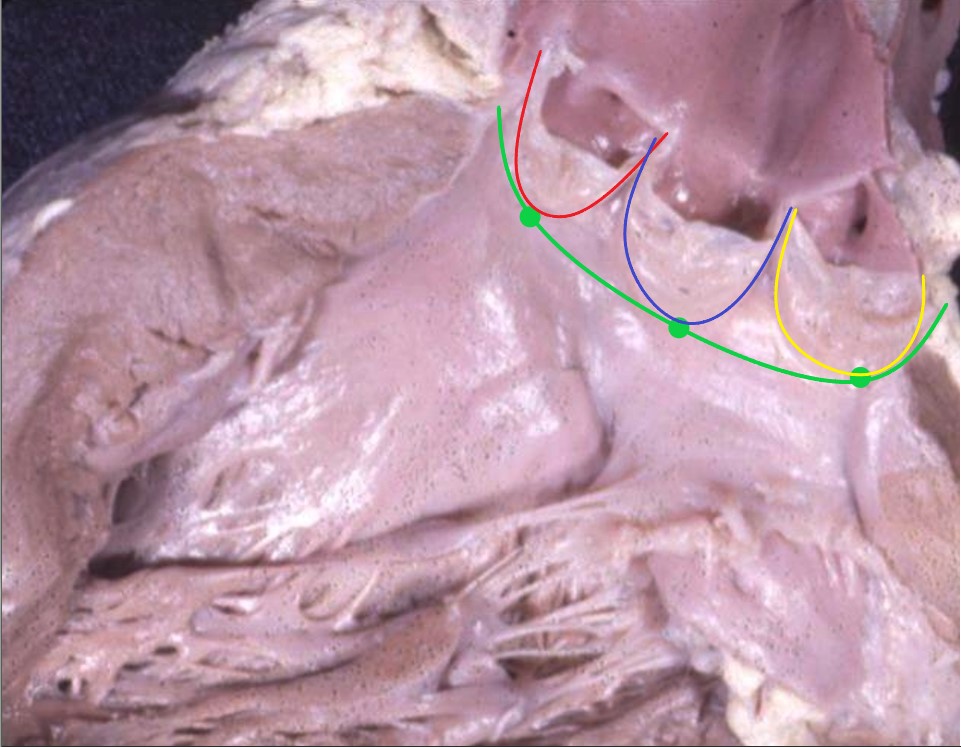
Hinge Points
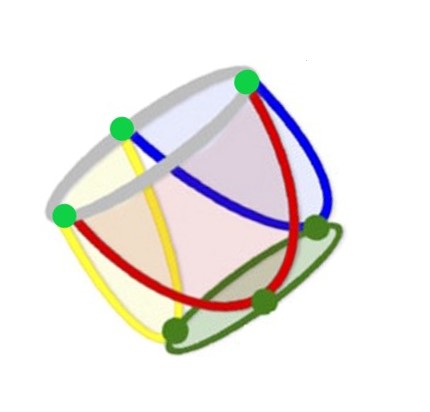
Each aortic leaflet is attached to the basal portion of the annulus (green sphere) by hinge points (green spheres Ashley Davidoff
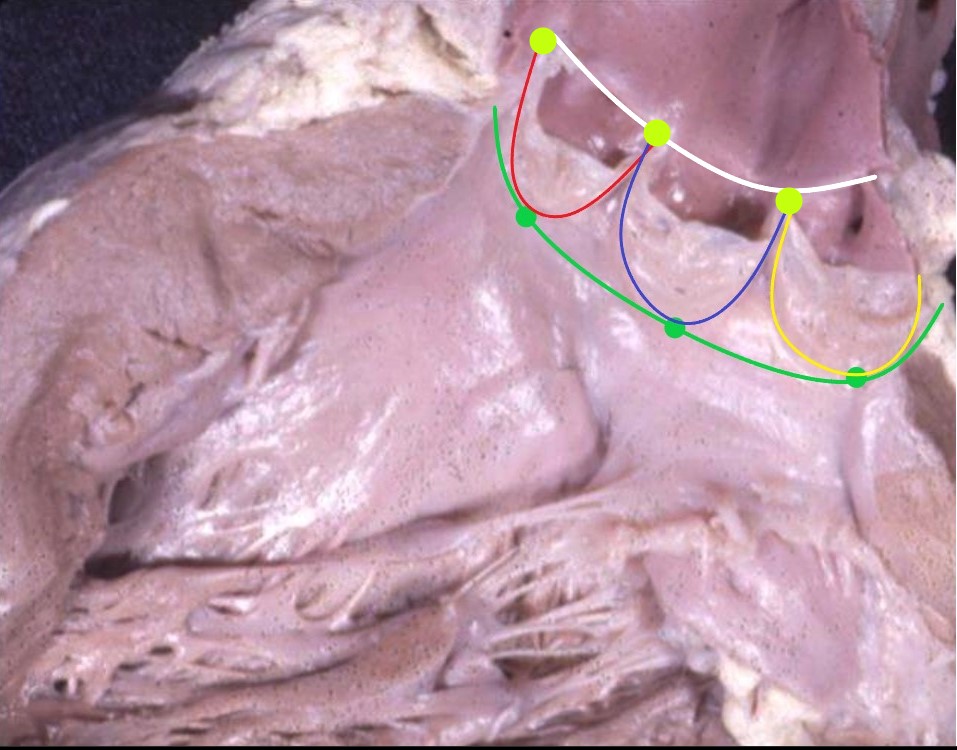
Commissures
The superior aspects of the junction points of the leaflets are attached to the sinotubular junction white line) at the commiissures (light green) Ashley Davidoff The Functional Aortic Annulus Each sinus is attached at a hinge point (dark green sphere) to the aortic annulus and attached to the region of the sino-tubular junction at the commissures (light green spheres Ashley Davidoff – Modified from diagram Patel P et al The Aortic Valve ? 3 cusps thickened at the Edges Forming Commissures and Sinuses and Attached to the Annulus (red) The aortic valve (AV) lies central to many structures including the right ventricular outflow tract (RVOT), pulmonary valve (PV), left atrium (LA), right atrium (RA), and superior vena cava (SVC). aorta from above. In this diagram, the commissures are overlaid in green, the crescent shaped lunulae reflect the free edge of the leaflets and are overlaid in yellow, and the nodules of Arantii are overlaid in orange. The sinuses of Valsalva are like cups and are positioned between the free edges. (gray) 47681d07 Ashley Davidoff MD
Annulus
Diameter 3 cms
The aortic annulus is part of the circulatory system and is the juncture between the ascending aorta and the aortic valve.
It is structurally characterized by its ring structure with a diameter of 3.0 cm.
The function of the aortic annulus is to act as a point of attachment for the aortic valve.
The most common diseases of the aortic annulus are calcified aortic sclerosis, syphilitic aortitis, and ring abscess.
The most commonly used diagnostic procedure for these diseases are CT scanning, fluorescent treponema antibody testing, and echocardiography, respectively.
These diseases are usually treated with antibiotics and surgery.
The aortic annulus is the ringed juncture of the outer wall of the aortic valve and ascending aorta. It is characterized structurally by its circular geometry, approximately3.0 cm in diameter. It acts as the foundation for the attachment of the aortic valve. The most common disease is calcified aortic sclerosis. As a distinct structure it is not easily appreciated by conventional imaging but when calcified for example in aortic sclerosis, it is easily seen by CT scanning. In the case of a ring abscess caused by bacterial endocarditis this entity is well seen by echocardiography. The abnormal sclerotic annulus itself is usually asymptomatic. When aortic sclerosis progresses with aortic stenosis to become severe, then surgical treatment by aortic valve replacement is warranted.
Aortic Sclerosis
Applied Biology
Aortic sclerosis is a degenerative disease commonly seen in older patients.
Aortic valve thickening (sclerosis) without stenosis is common in elderly adults often detected as a systolic murmur can progress to aortic stenosis with increased cardiovascular risk.
Predisposisng Facctors
hypertension and
electrocardiographic evidence of left ventricular hypertrophy
25% individuals ?65 years of age
65 %in those ages 75 to 84 years
Marker o atherosclerosis
Early
lipid accumulation, inflammation, and calcification similar to atherosclerosis
It results in the progressive calcification of the aortic annulus and/or aortic valve. This disease also induces thickening of the arterial wall. These effects cause heightened pressures in the left ventricle, increasing the risk of myocardial ischemia. The aortic annulus is prone to calcification because fatty acid deposits easily accumulate on the aortic surface at its junction with the valves. The detection of a calcified annulus by CTscan or transthoracic echocardiography indicates the diagnosis of aortic sclerosis. If severe, surgical treatment is required.
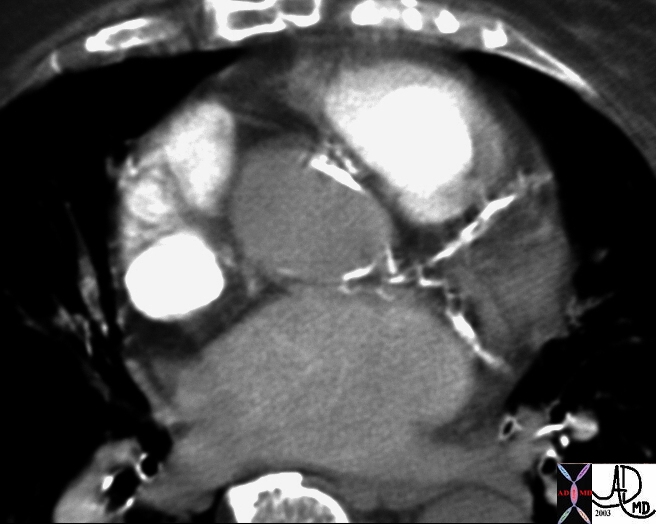
Calcified Aortic Annulus and Calcified Coronary Arteries This CTscan with contrast still within the right sided circulation shows heavy calcification of the left anterior descending artery, the circumflex coronary artery as well as calcification of the aortic annulus. Courtesy Ashley Davidoff MD. 15401
Ring Abscess
Ring Abscess is a suppurative infection of the annulus caused most frequently by infectious endocarditis. Such an infection is fatal if left untreated. In many cases, more than one microbial agent is responsible. The most common bacterial agents are E. coli and staphylococci. With degeneration of the endothelium overlying the annulus, deposition of platelets and fibrin occurs. This fibrous complex is nonbacterial at first, called nonbacterial thrombotic endocarditis. This structural defect can become colonized by bacteria and may progress to a ring abscess that requires drainage. A drained abscess may produce a false aneurysm of a sinus of Valsalva. A ring abscess is diagnosed by echocardiography. Surgical treatment involving excision and interposition grafting is a necessary to prevent further spread of infection and damage to the valve.
Ring Abscess of the Aorta
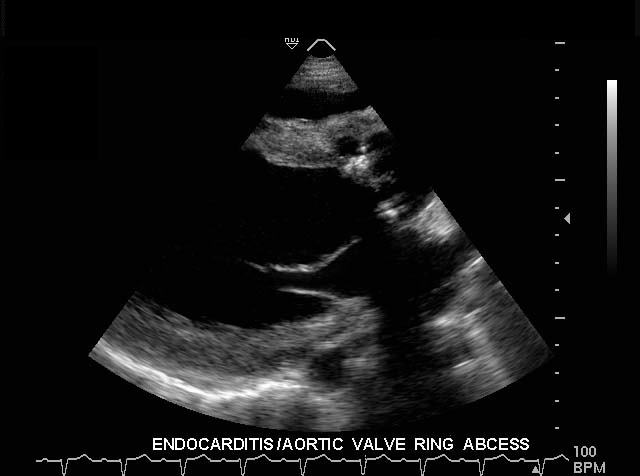
The first gray scale echo of the heart in long axis, shows the left ventricle, anterior and posterior leaflets of the mitral valve, the aortic valve and the base of the aorta. There is a rounded echogenic focus on the aortic valve ring together with a small fluid collection. In the setting of a febrile illness this represents a ring abscess complicating bacterial endocarditis. The ring abscess is better seen in the second image in transverse projection where two echogenic foci are seen associated with the fluid collection posteriorly.
Courtesy Philips Medical Systems 33133 33168
Syphilitic Aortitis
Syphilitic Aortitis is an infection of the aorta resulting from the tertiary or spirochetemic phase of primary syphilis. It commonly occurs at the site of the annulus, beginning as an inflammation of the vascular adventitia and vasa vasorum due to Treponema pallidum colonization. Necrosis follows as the adventia thickens, causing elastic fiber fragmentation and overall degeneration of the aortic wall. This condition makes the annulus susceptible to aneurysmal growth. A positive fluorescent treponema antibody test is a good indicator of the presence of syphilitic aortitis. If identified early, syphilitic aortitis can be treated by the administration of antibiotics such as penicillin. If complications or severe degeneracy and/or aortic aneurysm occurs, surgical treatment is necessary.
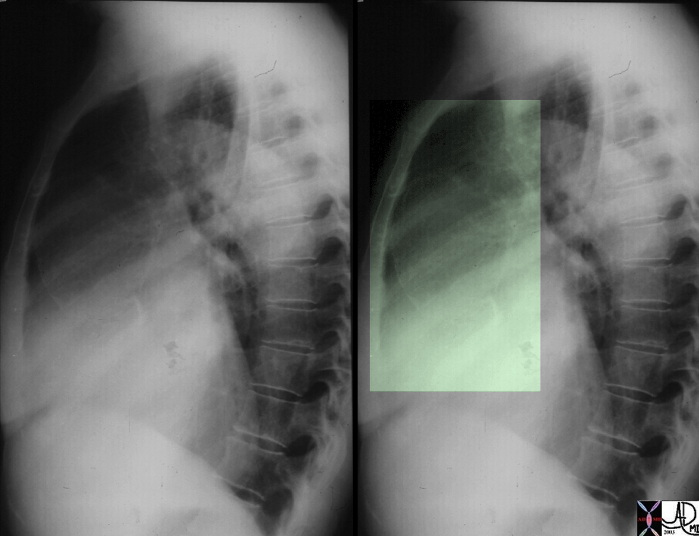
Syphilitic Aortitis
Effects are seen on the Annulus and Ascending Aorta
This lateral examination of the chest shows fine calcification in an ectatic ascending aorta associated with aortic annular calcification. Note the remarkable paucity of atherosclerotic change in the descending aorta. These findings are highly characteristic of tertiary syphilis of the aorta.
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => table
[nodeValue] =>
Syphilitic Aortitis
Effects are seen on the Annulus and Ascending Aorta
This lateral examination of the chest shows fine calcification in an ectatic ascending aorta associated with aortic annular calcification. Note the remarkable paucity of atherosclerotic change in the descending aorta. These findings are highly characteristic of tertiary syphilis of the aorta.
Courtesy Ashley Davidoff MD. 00018c code CVS artery aorta ascending syphilis aneurysm calcification tortoise shell
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Syphilitic Aortitis
Effects are seen on the Annulus and Ascending Aorta
This lateral examination of the chest shows fine calcification in an ectatic ascending aorta associated with aortic annular calcification. Note the remarkable paucity of atherosclerotic change in the descending aorta. These findings are highly characteristic of tertiary syphilis of the aorta.
Courtesy Ashley Davidoff MD. 00018c code CVS artery aorta ascending syphilis aneurysm calcification tortoise shell
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This lateral examination of the chest shows fine calcification in an ectatic ascending aorta associated with aortic annular calcification. Note the remarkable paucity of atherosclerotic change in the descending aorta. These findings are highly characteristic of tertiary syphilis of the aorta.
Courtesy Ashley Davidoff MD. 00018c code CVS artery aorta ascending syphilis aneurysm calcification tortoise shell
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This lateral examination of the chest shows fine calcification in an ectatic ascending aorta associated with aortic annular calcification. Note the remarkable paucity of atherosclerotic change in the descending aorta. These findings are highly characteristic of tertiary syphilis of the aorta.
Courtesy Ashley Davidoff MD. 00018c code CVS artery aorta ascending syphilis aneurysm calcification tortoise shell
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Syphilitic Aortitis
Effects are seen on the Annulus and Ascending Aorta
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Syphilitic Aortitis
Effects are seen on the Annulus and Ascending Aorta
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Ring Abscess of the Aorta
The first gray scale echo of the heart in long axis, shows the left ventricle, anterior and posterior leaflets of the mitral valve, the aortic valve and the base of the aorta. There is a rounded echogenic focus on the aortic valve ring together with a small fluid collection. In the setting of a febrile illness this represents a ring abscess complicating bacterial endocarditis. The ring abscess is better seen in the second image in transverse projection where two echogenic foci are seen associated with the fluid collection posteriorly.
Courtesy Philips Medical Systems 33133 33168
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Ring Abscess of the Aorta
The first gray scale echo of the heart in long axis, shows the left ventricle, anterior and posterior leaflets of the mitral valve, the aortic valve and the base of the aorta. There is a rounded echogenic focus on the aortic valve ring together with a small fluid collection. In the setting of a febrile illness this represents a ring abscess complicating bacterial endocarditis. The ring abscess is better seen in the second image in transverse projection where two echogenic foci are seen associated with the fluid collection posteriorly.
Courtesy Philips Medical Systems 33133 33168
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The first gray scale echo of the heart in long axis, shows the left ventricle, anterior and posterior leaflets of the mitral valve, the aortic valve and the base of the aorta. There is a rounded echogenic focus on the aortic valve ring together with a small fluid collection. In the setting of a febrile illness this represents a ring abscess complicating bacterial endocarditis. The ring abscess is better seen in the second image in transverse projection where two echogenic foci are seen associated with the fluid collection posteriorly.
Courtesy Philips Medical Systems 33133 33168
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The first gray scale echo of the heart in long axis, shows the left ventricle, anterior and posterior leaflets of the mitral valve, the aortic valve and the base of the aorta. There is a rounded echogenic focus on the aortic valve ring together with a small fluid collection. In the setting of a febrile illness this represents a ring abscess complicating bacterial endocarditis. The ring abscess is better seen in the second image in transverse projection where two echogenic foci are seen associated with the fluid collection posteriorly.
Courtesy Philips Medical Systems 33133 33168
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Ring Abscess of the Aorta
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Ring Abscess of the Aorta
)