Corpus Callosum
Sumit Karia MD Ashley Davidoff MD
The Common Vein
Copyright 2010
Definition
The corpus callosum is commissure that connects the two cerebral hemispheres; it contains four major subdivisions: rostrum, genu, body, and splenium. It is the largest of the brain’s commissures.
Structurally characterized by by its shape and position as it parallels the shape of the cortical components of the forebrain above it. It is composed of white matter axons under the cortex. Corpus means body and callosum means hard and it has a classical “hard carrot” like feel to its nature. The corpus callosum connects the hemispheres of the brain longitudinally.
It has a quadrilateral shape, measures between 8 to 10 cm in the longitudinal dimension; it has about 18 mm of transverse diameter in the superior face / 30-40 mm in the inferior face and 10-15 mm of height. Its superior face relates to the cerebral falx, cingulated gyrus and the pericallosal arteries. White and gray tracts can be seen. The inferior face relates with the fornix and septum pellucidum in the midline, and with the lateral ventricles in both sides. The anterior extremity has a curved shape, forming the genum, its most anterior part, the ?peak?, being called the rostrum. The posterior segment is free and rounded, being termed splenium. The posterior angles form fiber radiations called the forceps major of the corpus callosum which bend sharply backward into the occipital lobe of the cerebrum. Similarly, another set of fibers which are more external are called the tapetum. The anterior angles also form fiber radiations which bend forward toward the frontal pole of the cerebrum; this is called the forceps minor.
It is composed essentially by nerve fibers that travel transversely, which begin in a given point in one of the hemispheres and end in a symmetric point on the opposite hemisphere. Its function is thus to be a communication bridge between both hemispheres.
It functions to coordinate the activities of the hemispheres and much of the communication between hemispheres is faciliated by the corpus callosum. The corpus callosum may be responsible for conferring musical ability as musicians have been found to have larger corpus callosums than non musicians. The genum contains the fibers that bridge both frontal lobes. The splenium contains large bundles of fibers which connect the parietal lobes. The rostrum is composed of fibers that bridge the occipital lobes.
Specific diseases are not common in the corpus callosum but epilepsy is commommonly linked to the corpus callosum. Other diseases such as split brain or septo-optic displasia are characteristic but quite uncommon. Agenesis of the corpus callosum is a congenital birth defect associated with a single base pair substitution mutation. Panhypopituitarism can also result from abnormal corpus callosum development. In alcoholics, Marchiafava-Bignami disease can occur – caused by demyelinating lesions on the corpus callosum. Symptoms of the disease include depression, paranoia, psychosis, and dementia. Lesions on the corpus callosum after trauma leading to a coma have been correlated with the persistence of the vegetative state.
Since the dominant hemisphere regulates the activity of the dominated, a lesion in these commissural fibers impedes this regulation to occur. This results in an inability to produce complex voluntary movements (apraxia).
A lesion at level of the genum (contains fibers that conduct sensory information), for example, will result in astereognosis (inability to recognize objects by touch. Other sensory disorders may occur, for example, inability to repeat syllables when reading.
Diagnosis of disease is best accomplished by brain scan using MRI or CT in adults. During gestation, prenatal ultrasound or MRI are also utilized.
Treatment in epilepsy sometimes requires the corpus callosum to be severed to reduce epileptic seizures in patients in whom other treatments have been unsuccessful. Patients who undergo this procedure generally behave normally following the procedure. Developmental therapy is useful for children born with angenesis of the corpus callosum.

Corpus Callosum – Distinctive Shape, Position and White Color |
|
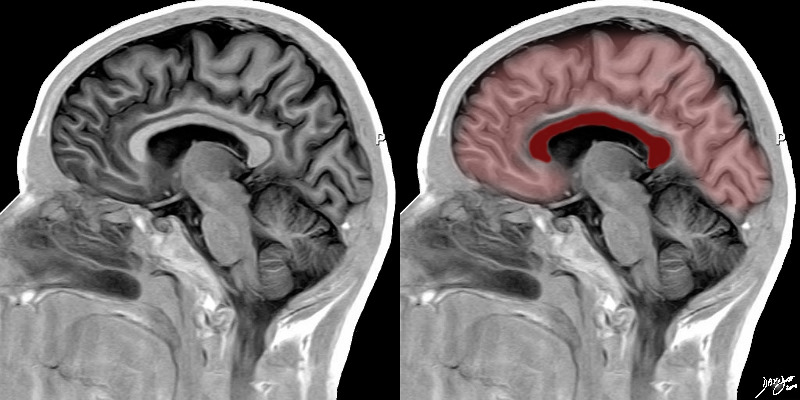
The midsagittal section view of brain reveals the distinctive shape position and character of the corpus callosum
The distinction between the character of the cerebral cortex which has a creamy color and the white matter exemplified by the corpus callosum (c) which is white, and the midbrain (mb) pons (p) and medulla (m) which are off white as opposed to the color of the cerebellum (c) which is light salmon pink is well demonstrated.
The relative sizes of the forebrain, midbrain and hindbrain are well appreciated in this section.
Image Courtesy of Thomas W.Smith, MD; Department of Pathology, University of Massachusetts Medical School. 97805b01
|
|
Corpus Callosum 49079b05b03 |
| 49079b05b03 brain cerebrum cerebral corpus callosum normal anatomy MRI T1 weighted sagital Davidoff MD |
|
 
Corpus Callosum |
| 49079 Brain Normal Frontal lobe pariental lobe temporal lobe Cerebellum lateral ventricle fourth ventricle Pons Thalamus cerebral aqueduct genu corpus callosum 61 Male T1 sagital Courtesy Ashley Davidoff MD Uploaded RP
71431.800 brain cerebral anatomy corpus callosum third ventricle occipital lobe basilar artery pons cerebellum pons cerebellum normal MRI T2 weighted images |
|
92170c03.8s
|
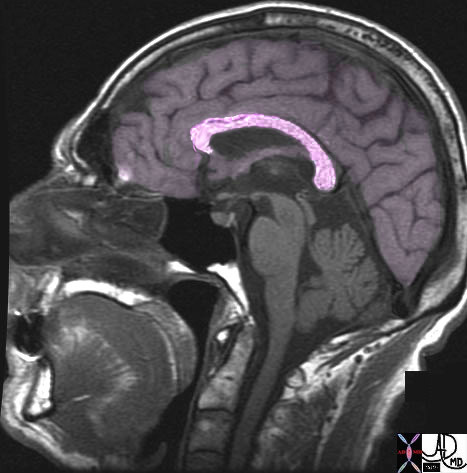
| 92170c03.8s The inversion recovery MRI sagittal section through the midline of the brain shows the forebrain superiorly and the corpus callosum (maroon) parralleling the course of the forebrain lying inferiorly code brain forebrain corpus callosum MRI inversion recovery proton density Images provided by Philips Medical Systems Modified and artictically rendered by Davidoff art copyright 2010 all rights reserved |
Genu and Splenium at a Lower Level
|
|
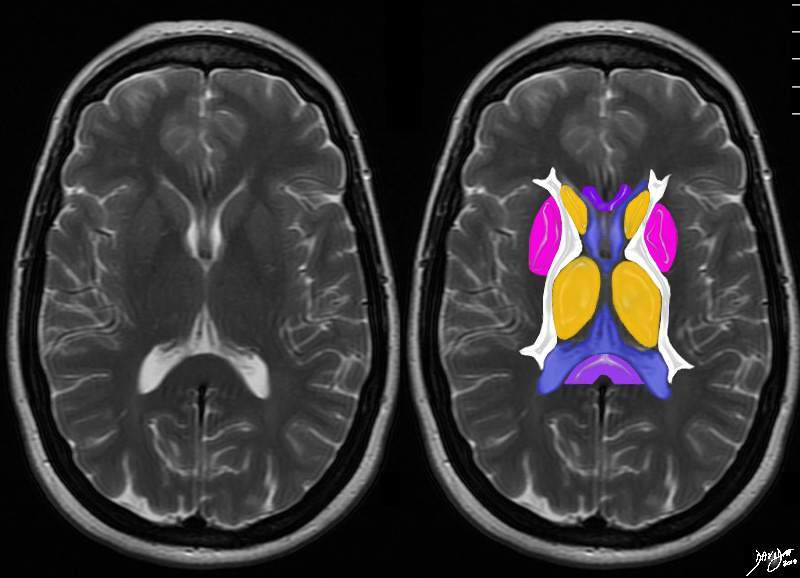
The axial T2 weighted MRI is taken through the level of the ventricles. The body of the corpus callosum is above this level. The most anterior portion of the corpus callosum and most posterior portion are seen at this lower level of the ventricles
Courtesy Ashley Davidoff MD copyright 2010 all rights reserved 94079c04b05.8s
|
Neonatal Corpus Callosum by Ultrasound |
|
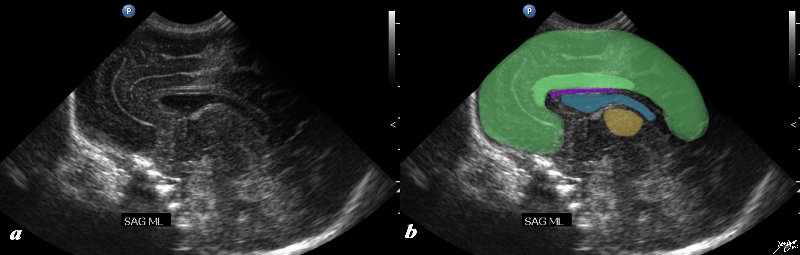
The ultrasound of a 7 day old baby boy reveals a normal sagittal section through the brain showing the CSF filled lateral ventricle (light blue) with most the brain substance showing characteristic homogeneous solid organ texture. The echogenic interfaces of the sulci with the gyri enable the outline of characteristic forms of the gyri so that for example the cingulate gyrus (darker green) is easily recognized by its classical location above the corpus callosum (purple). The corpus callosum is hypoechoic and overlaid in purple. The thalamus is isoechoic (orange) recognized by its position and shape rather than any unique ultrasound characteristics. The forebrain including the frontal parietal and temporal lobes are overlaid in green
Courtesy Ashley Davidoff MD Copyright 2010 90986c02.8s
|
|
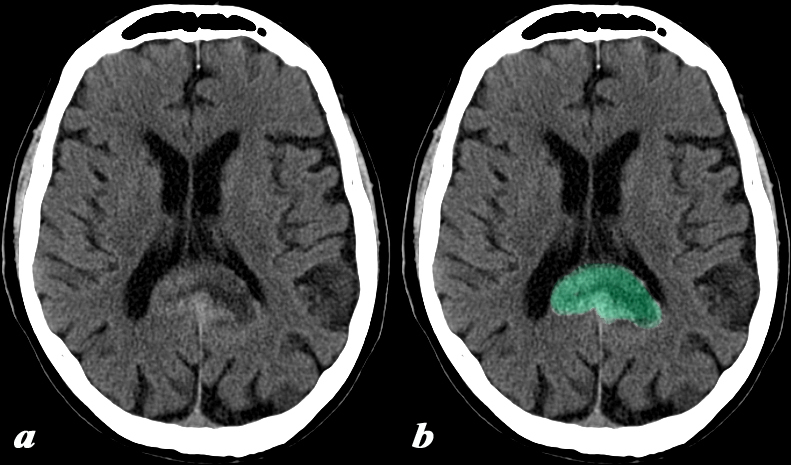
GBM in the Splenium |
|
This 74 year old male presented with memory impairment and confusion.
CT: (a,b)
This head CT obtained without contrast demonstrates irregular enlargement of the splenium of the corpus callosum which has abnormal decreased central and increased peripheral density (green b), and crosses the midline. These findings are consistent with a diagnosis of glioblastoma multiforme. Included in the differential diagnosis for lesions crossing the midline is primary lymphoma of the brain code
Image Courtesy Elisa Flower MD and Asim Mian MD 97644c.8
|
|
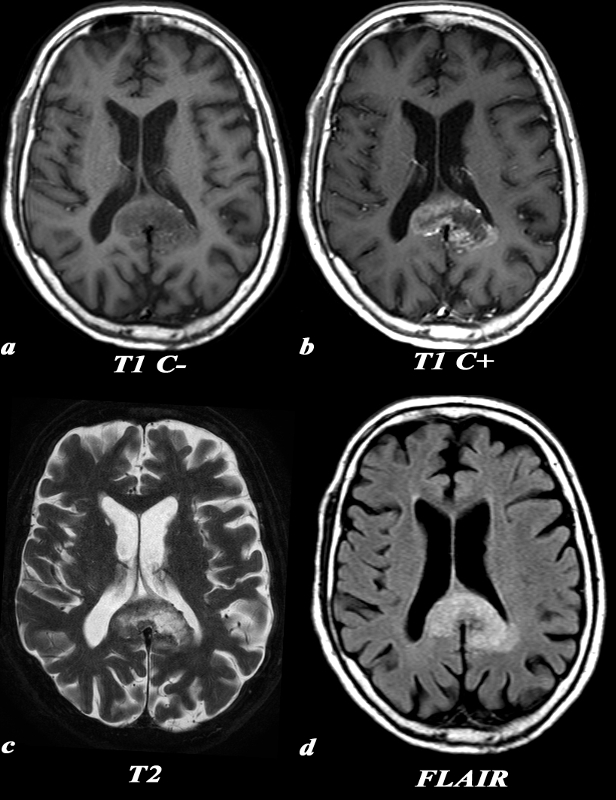
MRI GBM |
|
This 74 year old male presented with memory impairment and confusion. A previously performed head CT had shown a space occupying lesion in the splenium of the corpus callosum (above).
MRI: (a,b,c,d) T1 weighted axial images before contrast (a) demonstrates a low signal in the enlarged splenium of the corpus callosum. The post contrast T1 weighted image (b) in the axial plane demonstrates the peripheral and irregular enhancement of the mass. This configuration is classic and often called a ?butterfly? glioma.
Remember that due to the infiltrative nature of the mass, the extent of actual tumor involvement is larger than what is demonstrated by imaging on the post contrast images. This lesion which is hyperintense on T2 (c), enlarges the splenium, crosses the midline and involves the medial aspect of the left parietal lobe. Similar findings are identified on the FLAIR image. The extension into the parietal lobe is best seen on the FLAIR image
These findings are consistent with a diagnosis of glioblastoma multiforme. Included in the differential diagnosis for lesions crossing the midline is primary lymphoma of the brain
Image Courtesy Elisa Flower MD and Asim Mian MD 97647c01.8
|
|
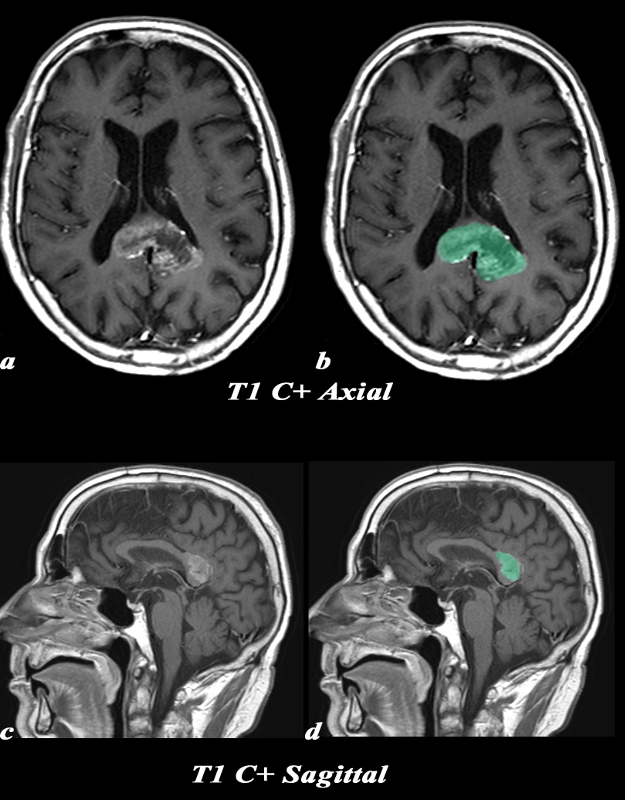
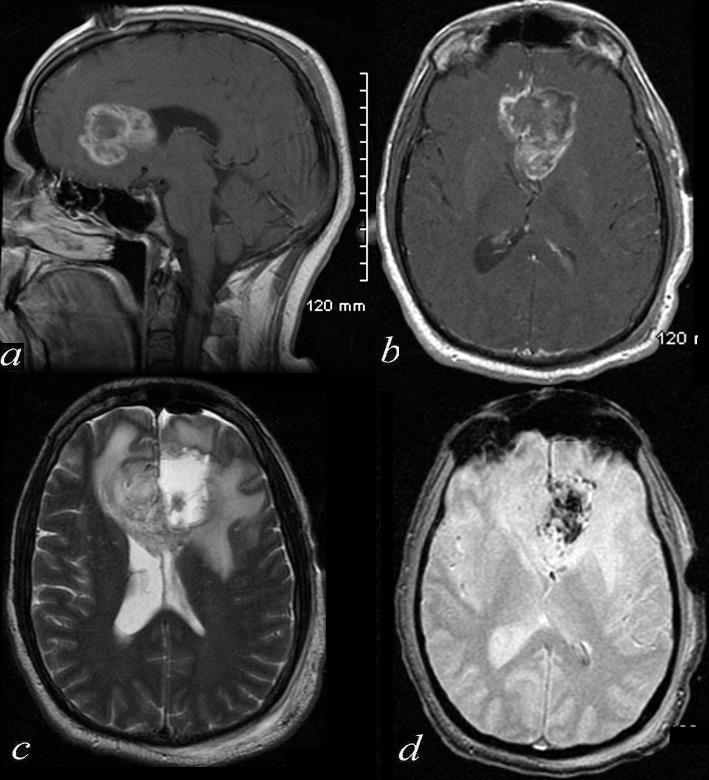
GBM – Axial and Sagittal
|
|
This 74 year old male presented with memory impairment and confusion. A previously performed head CT had shown a space occupying lesion in the splenium of the corpus callosum.
MRI: (a,b,c,d) T1 weighted axial images after contrast (a) demonstrates peripheral and irregular enhancement of the mass overlaid in green in b,. This configuration is classic and often called a ?butterfly? glioma. Remember that due to the infiltrative nature of the mass, the extent of actual tumor involvement is larger than what is demonstrated by imaging on the post contrast images. The sagittal image(c,d) is a T1 weighted sequence following gadolinium and shows that the lesion is originating from the splenium of the corpus callosum. These findings are consistent with a diagnosis of glioblastoma multiforme. Included in the differential diagnosis for lesions crossing the midline is primary lymphoma of the brain
Image Courtesy Elisa Flower MD and Asim Mian MD 97647c02.8
|
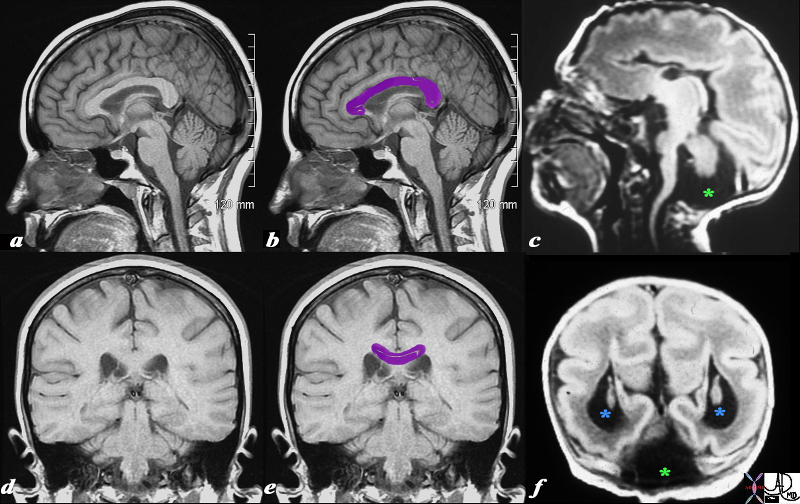
Normal and Congenital Absence of the Corpus Callosum associated with
Lissencephaly and Dandy-Walker Syndrome |
|
This T1 weighted MRI is from a normal patient juxtaposed on a T1 weighted MRI from a neonate with agenesis of the corpus callosum, congenital lissencephaly and Dandy Walker syndrome. The normal corpus callosum (purple overlay ) is seen above the ventricles between the ventricles and the supracallosul gyrus and cingulate gyrus. . In the neonate (c,f) the there is no white matter in the expected position of the corpus callosum. These findings are consistent with a diagnosis of agenesis of the corpus callosum In addition, the posterior fossa does not show a normal cerebellum. Instead it is mostly filled with CSF (dark T1 green asterisk) likely due to a dilated 4th ventricle and atrophy of the vermis. Only a small amount of posterior fossa soft tissue is seen. In addition the posterior horns are dilated (blue asterisk). This finding is consistent with a diagnosis of Dandy-Walker syndrome associated with hydrocephalus. Lastly the patient has fewer gyri and sulci than normal. The gyri that are present are also more shallow than normal. These findings are consistent with lissencephaly.
Courtesy James Donnelly MD Copyright 2010 All rights reserved 95466c01L03.8s
|
| Pericallosal Lipoma and Partial Agenesis of the Corpus Callosum |
|
This 65 year old female was noted to have a large pericallosal lipoma.
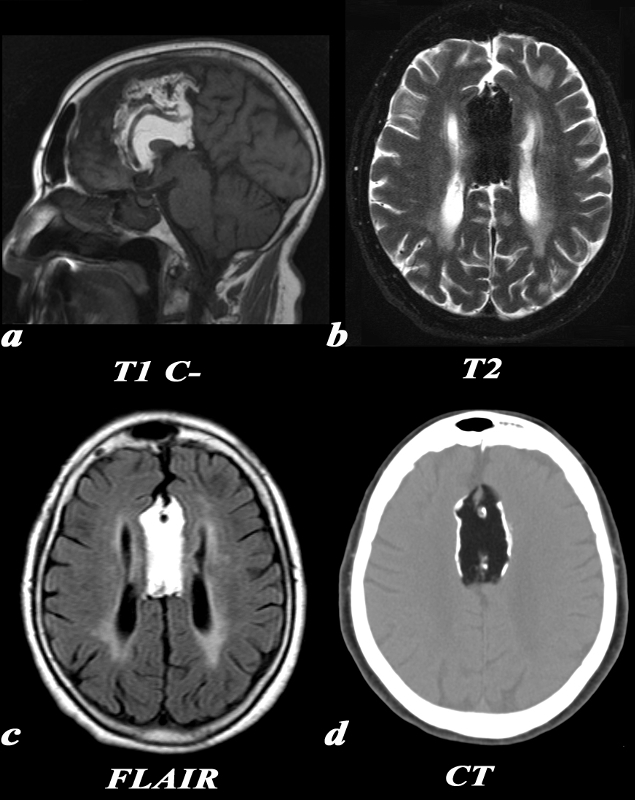
MRI, T1 (a): The large pericallosal lipoma is T1 hyperintense and follows the signal intensity of fat. There is partial agenesis of the corpus callosum, with only the genu being visualized on this midline sagittal image. Also note the anterior cerebral arteries coursing directly through the lipoma
T2 (b): This T2 weighted image is obtained using a technique which suppresses fat. The signal within the lipoma has been suppressed causing it to be hypointense.
FLAIR (c): On this FLAIR sequence, again note that the signal in the lesion follows that of fat signal. Also note the parallel configuration of the lateral ventricles consistent with partial agenesis of the corpus callosum.
CT (d): On CT, the low density matches that of the subcutaneous fat. This lipoma has peripheral calcification.
The diagnosis is consistent with a pericallosal lipoma with peripheral calcification and partial agenesis of the corpus callosum
Image Courtesy Elisa Flower MD and Asim Mian MD 97660c.8
|
|
Glioblastoma of the Corpus Callosum S/P Debulking
|
| 72420c01 46 male brain cerebrum genu of the corpus callosum crosses midline enhancing tumor in periphery surrounding edema dilated right hor mass effect on the lateral ventricles tumor arises from the corpus callosum post operative resection of the left side of the tumor methemoglobin effects in the left side a = T1 post gadolinium b= T1 weighted post contrast c= T2 weighted d = GRE blood products T2* effects dx glioblastoma s/p debulking Davidoff MD |
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Glioblastoma of the Corpus Callosum S/P Debulking
72420c01 46 male brain cerebrum genu of the corpus callosum crosses midline enhancing tumor in periphery surrounding edema dilated right hor mass effect on the lateral ventricles tumor arises from the corpus callosum post operative resection of the left side of the tumor methemoglobin effects in the left side a = T1 post gadolinium b= T1 weighted post contrast c= T2 weighted d = GRE blood products T2* effects dx glioblastoma s/p debulking Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Glioblastoma of the Corpus Callosum S/P Debulking
72420c01 46 male brain cerebrum genu of the corpus callosum crosses midline enhancing tumor in periphery surrounding edema dilated right hor mass effect on the lateral ventricles tumor arises from the corpus callosum post operative resection of the left side of the tumor methemoglobin effects in the left side a = T1 post gadolinium b= T1 weighted post contrast c= T2 weighted d = GRE blood products T2* effects dx glioblastoma s/p debulking Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 72420c01 46 male brain cerebrum genu of the corpus callosum crosses midline enhancing tumor in periphery surrounding edema dilated right hor mass effect on the lateral ventricles tumor arises from the corpus callosum post operative resection of the left side of the tumor methemoglobin effects in the left side a = T1 post gadolinium b= T1 weighted post contrast c= T2 weighted d = GRE blood products T2* effects dx glioblastoma s/p debulking Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 72420c01 46 male brain cerebrum genu of the corpus callosum crosses midline enhancing tumor in periphery surrounding edema dilated right hor mass effect on the lateral ventricles tumor arises from the corpus callosum post operative resection of the left side of the tumor methemoglobin effects in the left side a = T1 post gadolinium b= T1 weighted post contrast c= T2 weighted d = GRE blood products T2* effects dx glioblastoma s/p debulking Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Glioblastoma of the Corpus Callosum S/P Debulking
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Glioblastoma of the Corpus Callosum S/P Debulking
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Pericallosal Lipoma and Partial Agenesis of the Corpus Callosum
This 65 year old female was noted to have a large pericallosal lipoma.
MRI, T1 (a): The large pericallosal lipoma is T1 hyperintense and follows the signal intensity of fat. There is partial agenesis of the corpus callosum, with only the genu being visualized on this midline sagittal image. Also note the anterior cerebral arteries coursing directly through the lipoma
T2 (b): This T2 weighted image is obtained using a technique which suppresses fat. The signal within the lipoma has been suppressed causing it to be hypointense.
FLAIR (c): On this FLAIR sequence, again note that the signal in the lesion follows that of fat signal. Also note the parallel configuration of the lateral ventricles consistent with partial agenesis of the corpus callosum.
CT (d): On CT, the low density matches that of the subcutaneous fat. This lipoma has peripheral calcification.
The diagnosis is consistent with a pericallosal lipoma with peripheral calcification and partial agenesis of the corpus callosum
Image Courtesy Elisa Flower MD and Asim Mian MD 97660c.8
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Pericallosal Lipoma and Partial Agenesis of the Corpus Callosum
This 65 year old female was noted to have a large pericallosal lipoma.
MRI, T1 (a): The large pericallosal lipoma is T1 hyperintense and follows the signal intensity of fat. There is partial agenesis of the corpus callosum, with only the genu being visualized on this midline sagittal image. Also note the anterior cerebral arteries coursing directly through the lipoma
T2 (b): This T2 weighted image is obtained using a technique which suppresses fat. The signal within the lipoma has been suppressed causing it to be hypointense.
FLAIR (c): On this FLAIR sequence, again note that the signal in the lesion follows that of fat signal. Also note the parallel configuration of the lateral ventricles consistent with partial agenesis of the corpus callosum.
CT (d): On CT, the low density matches that of the subcutaneous fat. This lipoma has peripheral calcification.
The diagnosis is consistent with a pericallosal lipoma with peripheral calcification and partial agenesis of the corpus callosum
Image Courtesy Elisa Flower MD and Asim Mian MD 97660c.8
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 7
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
This 65 year old female was noted to have a large pericallosal lipoma.
MRI, T1 (a): The large pericallosal lipoma is T1 hyperintense and follows the signal intensity of fat. There is partial agenesis of the corpus callosum, with only the genu being visualized on this midline sagittal image. Also note the anterior cerebral arteries coursing directly through the lipoma
T2 (b): This T2 weighted image is obtained using a technique which suppresses fat. The signal within the lipoma has been suppressed causing it to be hypointense.
FLAIR (c): On this FLAIR sequence, again note that the signal in the lesion follows that of fat signal. Also note the parallel configuration of the lateral ventricles consistent with partial agenesis of the corpus callosum.
CT (d): On CT, the low density matches that of the subcutaneous fat. This lipoma has peripheral calcification.
The diagnosis is consistent with a pericallosal lipoma with peripheral calcification and partial agenesis of the corpus callosum
Image Courtesy Elisa Flower MD and Asim Mian MD 97660c.8
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
This 65 year old female was noted to have a large pericallosal lipoma.
MRI, T1 (a): The large pericallosal lipoma is T1 hyperintense and follows the signal intensity of fat. There is partial agenesis of the corpus callosum, with only the genu being visualized on this midline sagittal image. Also note the anterior cerebral arteries coursing directly through the lipoma
T2 (b): This T2 weighted image is obtained using a technique which suppresses fat. The signal within the lipoma has been suppressed causing it to be hypointense.
FLAIR (c): On this FLAIR sequence, again note that the signal in the lesion follows that of fat signal. Also note the parallel configuration of the lateral ventricles consistent with partial agenesis of the corpus callosum.
CT (d): On CT, the low density matches that of the subcutaneous fat. This lipoma has peripheral calcification.
The diagnosis is consistent with a pericallosal lipoma with peripheral calcification and partial agenesis of the corpus callosum
Image Courtesy Elisa Flower MD and Asim Mian MD 97660c.8
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => Pericallosal Lipoma and Partial Agenesis of the Corpus Callosum
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => Pericallosal Lipoma and Partial Agenesis of the Corpus Callosum
)
https://beta.thecommonvein.net/wp-content/uploads/2023/05/97660c.8.jpg
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Normal and Congenital Absence of the Corpus Callosum associated with
Lissencephaly and Dandy-Walker Syndrome
This T1 weighted MRI is from a normal patient juxtaposed on a T1 weighted MRI from a neonate with agenesis of the corpus callosum, congenital lissencephaly and Dandy Walker syndrome. The normal corpus callosum (purple overlay ) is seen above the ventricles between the ventricles and the supracallosul gyrus and cingulate gyrus. . In the neonate (c,f) the there is no white matter in the expected position of the corpus callosum. These findings are consistent with a diagnosis of agenesis of the corpus callosum In addition, the posterior fossa does not show a normal cerebellum. Instead it is mostly filled with CSF (dark T1 green asterisk) likely due to a dilated 4th ventricle and atrophy of the vermis. Only a small amount of posterior fossa soft tissue is seen. In addition the posterior horns are dilated (blue asterisk). This finding is consistent with a diagnosis of Dandy-Walker syndrome associated with hydrocephalus. Lastly the patient has fewer gyri and sulci than normal. The gyri that are present are also more shallow than normal. These findings are consistent with lissencephaly.
Courtesy James Donnelly MD Copyright 2010 All rights reserved 95466c01L03.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Normal and Congenital Absence of the Corpus Callosum associated with
Lissencephaly and Dandy-Walker Syndrome
This T1 weighted MRI is from a normal patient juxtaposed on a T1 weighted MRI from a neonate with agenesis of the corpus callosum, congenital lissencephaly and Dandy Walker syndrome. The normal corpus callosum (purple overlay ) is seen above the ventricles between the ventricles and the supracallosul gyrus and cingulate gyrus. . In the neonate (c,f) the there is no white matter in the expected position of the corpus callosum. These findings are consistent with a diagnosis of agenesis of the corpus callosum In addition, the posterior fossa does not show a normal cerebellum. Instead it is mostly filled with CSF (dark T1 green asterisk) likely due to a dilated 4th ventricle and atrophy of the vermis. Only a small amount of posterior fossa soft tissue is seen. In addition the posterior horns are dilated (blue asterisk). This finding is consistent with a diagnosis of Dandy-Walker syndrome associated with hydrocephalus. Lastly the patient has fewer gyri and sulci than normal. The gyri that are present are also more shallow than normal. These findings are consistent with lissencephaly.
Courtesy James Donnelly MD Copyright 2010 All rights reserved 95466c01L03.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
This T1 weighted MRI is from a normal patient juxtaposed on a T1 weighted MRI from a neonate with agenesis of the corpus callosum, congenital lissencephaly and Dandy Walker syndrome. The normal corpus callosum (purple overlay ) is seen above the ventricles between the ventricles and the supracallosul gyrus and cingulate gyrus. . In the neonate (c,f) the there is no white matter in the expected position of the corpus callosum. These findings are consistent with a diagnosis of agenesis of the corpus callosum In addition, the posterior fossa does not show a normal cerebellum. Instead it is mostly filled with CSF (dark T1 green asterisk) likely due to a dilated 4th ventricle and atrophy of the vermis. Only a small amount of posterior fossa soft tissue is seen. In addition the posterior horns are dilated (blue asterisk). This finding is consistent with a diagnosis of Dandy-Walker syndrome associated with hydrocephalus. Lastly the patient has fewer gyri and sulci than normal. The gyri that are present are also more shallow than normal. These findings are consistent with lissencephaly.
Courtesy James Donnelly MD Copyright 2010 All rights reserved 95466c01L03.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
This T1 weighted MRI is from a normal patient juxtaposed on a T1 weighted MRI from a neonate with agenesis of the corpus callosum, congenital lissencephaly and Dandy Walker syndrome. The normal corpus callosum (purple overlay ) is seen above the ventricles between the ventricles and the supracallosul gyrus and cingulate gyrus. . In the neonate (c,f) the there is no white matter in the expected position of the corpus callosum. These findings are consistent with a diagnosis of agenesis of the corpus callosum In addition, the posterior fossa does not show a normal cerebellum. Instead it is mostly filled with CSF (dark T1 green asterisk) likely due to a dilated 4th ventricle and atrophy of the vermis. Only a small amount of posterior fossa soft tissue is seen. In addition the posterior horns are dilated (blue asterisk). This finding is consistent with a diagnosis of Dandy-Walker syndrome associated with hydrocephalus. Lastly the patient has fewer gyri and sulci than normal. The gyri that are present are also more shallow than normal. These findings are consistent with lissencephaly.
Courtesy James Donnelly MD Copyright 2010 All rights reserved 95466c01L03.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Normal and Congenital Absence of the Corpus Callosum associated with
Lissencephaly and Dandy-Walker Syndrome
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Normal and Congenital Absence of the Corpus Callosum associated with
Lissencephaly and Dandy-Walker Syndrome
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
GBM – Axial and Sagittal
This 74 year old male presented with memory impairment and confusion. A previously performed head CT had shown a space occupying lesion in the splenium of the corpus callosum.
MRI: (a,b,c,d) T1 weighted axial images after contrast (a) demonstrates peripheral and irregular enhancement of the mass overlaid in green in b,. This configuration is classic and often called a ?butterfly? glioma. Remember that due to the infiltrative nature of the mass, the extent of actual tumor involvement is larger than what is demonstrated by imaging on the post contrast images. The sagittal image(c,d) is a T1 weighted sequence following gadolinium and shows that the lesion is originating from the splenium of the corpus callosum. These findings are consistent with a diagnosis of glioblastoma multiforme. Included in the differential diagnosis for lesions crossing the midline is primary lymphoma of the brain
Image Courtesy Elisa Flower MD and Asim Mian MD 97647c02.8
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
GBM – Axial and Sagittal
This 74 year old male presented with memory impairment and confusion. A previously performed head CT had shown a space occupying lesion in the splenium of the corpus callosum.
MRI: (a,b,c,d) T1 weighted axial images after contrast (a) demonstrates peripheral and irregular enhancement of the mass overlaid in green in b,. This configuration is classic and often called a ?butterfly? glioma. Remember that due to the infiltrative nature of the mass, the extent of actual tumor involvement is larger than what is demonstrated by imaging on the post contrast images. The sagittal image(c,d) is a T1 weighted sequence following gadolinium and shows that the lesion is originating from the splenium of the corpus callosum. These findings are consistent with a diagnosis of glioblastoma multiforme. Included in the differential diagnosis for lesions crossing the midline is primary lymphoma of the brain
Image Courtesy Elisa Flower MD and Asim Mian MD 97647c02.8
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
This 74 year old male presented with memory impairment and confusion. A previously performed head CT had shown a space occupying lesion in the splenium of the corpus callosum.
MRI: (a,b,c,d) T1 weighted axial images after contrast (a) demonstrates peripheral and irregular enhancement of the mass overlaid in green in b,. This configuration is classic and often called a ?butterfly? glioma. Remember that due to the infiltrative nature of the mass, the extent of actual tumor involvement is larger than what is demonstrated by imaging on the post contrast images. The sagittal image(c,d) is a T1 weighted sequence following gadolinium and shows that the lesion is originating from the splenium of the corpus callosum. These findings are consistent with a diagnosis of glioblastoma multiforme. Included in the differential diagnosis for lesions crossing the midline is primary lymphoma of the brain
Image Courtesy Elisa Flower MD and Asim Mian MD 97647c02.8
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
This 74 year old male presented with memory impairment and confusion. A previously performed head CT had shown a space occupying lesion in the splenium of the corpus callosum.
MRI: (a,b,c,d) T1 weighted axial images after contrast (a) demonstrates peripheral and irregular enhancement of the mass overlaid in green in b,. This configuration is classic and often called a ?butterfly? glioma. Remember that due to the infiltrative nature of the mass, the extent of actual tumor involvement is larger than what is demonstrated by imaging on the post contrast images. The sagittal image(c,d) is a T1 weighted sequence following gadolinium and shows that the lesion is originating from the splenium of the corpus callosum. These findings are consistent with a diagnosis of glioblastoma multiforme. Included in the differential diagnosis for lesions crossing the midline is primary lymphoma of the brain
Image Courtesy Elisa Flower MD and Asim Mian MD 97647c02.8
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
GBM – Axial and Sagittal
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
GBM – Axial and Sagittal
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
MRI GBM
This 74 year old male presented with memory impairment and confusion. A previously performed head CT had shown a space occupying lesion in the splenium of the corpus callosum (above).
MRI: (a,b,c,d) T1 weighted axial images before contrast (a) demonstrates a low signal in the enlarged splenium of the corpus callosum. The post contrast T1 weighted image (b) in the axial plane demonstrates the peripheral and irregular enhancement of the mass. This configuration is classic and often called a ?butterfly? glioma.
Remember that due to the infiltrative nature of the mass, the extent of actual tumor involvement is larger than what is demonstrated by imaging on the post contrast images. This lesion which is hyperintense on T2 (c), enlarges the splenium, crosses the midline and involves the medial aspect of the left parietal lobe. Similar findings are identified on the FLAIR image. The extension into the parietal lobe is best seen on the FLAIR image
These findings are consistent with a diagnosis of glioblastoma multiforme. Included in the differential diagnosis for lesions crossing the midline is primary lymphoma of the brain
Image Courtesy Elisa Flower MD and Asim Mian MD 97647c01.8
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
MRI GBM
This 74 year old male presented with memory impairment and confusion. A previously performed head CT had shown a space occupying lesion in the splenium of the corpus callosum (above).
MRI: (a,b,c,d) T1 weighted axial images before contrast (a) demonstrates a low signal in the enlarged splenium of the corpus callosum. The post contrast T1 weighted image (b) in the axial plane demonstrates the peripheral and irregular enhancement of the mass. This configuration is classic and often called a ?butterfly? glioma.
Remember that due to the infiltrative nature of the mass, the extent of actual tumor involvement is larger than what is demonstrated by imaging on the post contrast images. This lesion which is hyperintense on T2 (c), enlarges the splenium, crosses the midline and involves the medial aspect of the left parietal lobe. Similar findings are identified on the FLAIR image. The extension into the parietal lobe is best seen on the FLAIR image
These findings are consistent with a diagnosis of glioblastoma multiforme. Included in the differential diagnosis for lesions crossing the midline is primary lymphoma of the brain
Image Courtesy Elisa Flower MD and Asim Mian MD 97647c01.8
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 5
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
This 74 year old male presented with memory impairment and confusion. A previously performed head CT had shown a space occupying lesion in the splenium of the corpus callosum (above).
MRI: (a,b,c,d) T1 weighted axial images before contrast (a) demonstrates a low signal in the enlarged splenium of the corpus callosum. The post contrast T1 weighted image (b) in the axial plane demonstrates the peripheral and irregular enhancement of the mass. This configuration is classic and often called a ?butterfly? glioma.
Remember that due to the infiltrative nature of the mass, the extent of actual tumor involvement is larger than what is demonstrated by imaging on the post contrast images. This lesion which is hyperintense on T2 (c), enlarges the splenium, crosses the midline and involves the medial aspect of the left parietal lobe. Similar findings are identified on the FLAIR image. The extension into the parietal lobe is best seen on the FLAIR image
These findings are consistent with a diagnosis of glioblastoma multiforme. Included in the differential diagnosis for lesions crossing the midline is primary lymphoma of the brain
Image Courtesy Elisa Flower MD and Asim Mian MD 97647c01.8
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
This 74 year old male presented with memory impairment and confusion. A previously performed head CT had shown a space occupying lesion in the splenium of the corpus callosum (above).
MRI: (a,b,c,d) T1 weighted axial images before contrast (a) demonstrates a low signal in the enlarged splenium of the corpus callosum. The post contrast T1 weighted image (b) in the axial plane demonstrates the peripheral and irregular enhancement of the mass. This configuration is classic and often called a ?butterfly? glioma.
Remember that due to the infiltrative nature of the mass, the extent of actual tumor involvement is larger than what is demonstrated by imaging on the post contrast images. This lesion which is hyperintense on T2 (c), enlarges the splenium, crosses the midline and involves the medial aspect of the left parietal lobe. Similar findings are identified on the FLAIR image. The extension into the parietal lobe is best seen on the FLAIR image
These findings are consistent with a diagnosis of glioblastoma multiforme. Included in the differential diagnosis for lesions crossing the midline is primary lymphoma of the brain
Image Courtesy Elisa Flower MD and Asim Mian MD 97647c01.8
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
MRI GBM
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
MRI GBM
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
GBM in the Splenium
This 74 year old male presented with memory impairment and confusion.
CT: (a,b)
This head CT obtained without contrast demonstrates irregular enlargement of the splenium of the corpus callosum which has abnormal decreased central and increased peripheral density (green b), and crosses the midline. These findings are consistent with a diagnosis of glioblastoma multiforme. Included in the differential diagnosis for lesions crossing the midline is primary lymphoma of the brain code
Image Courtesy Elisa Flower MD and Asim Mian MD 97644c.8
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
GBM in the Splenium
This 74 year old male presented with memory impairment and confusion.
CT: (a,b)
This head CT obtained without contrast demonstrates irregular enlargement of the splenium of the corpus callosum which has abnormal decreased central and increased peripheral density (green b), and crosses the midline. These findings are consistent with a diagnosis of glioblastoma multiforme. Included in the differential diagnosis for lesions crossing the midline is primary lymphoma of the brain code
Image Courtesy Elisa Flower MD and Asim Mian MD 97644c.8
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 4
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
This 74 year old male presented with memory impairment and confusion.
CT: (a,b)
This head CT obtained without contrast demonstrates irregular enlargement of the splenium of the corpus callosum which has abnormal decreased central and increased peripheral density (green b), and crosses the midline. These findings are consistent with a diagnosis of glioblastoma multiforme. Included in the differential diagnosis for lesions crossing the midline is primary lymphoma of the brain code
Image Courtesy Elisa Flower MD and Asim Mian MD 97644c.8
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
This 74 year old male presented with memory impairment and confusion.
CT: (a,b)
This head CT obtained without contrast demonstrates irregular enlargement of the splenium of the corpus callosum which has abnormal decreased central and increased peripheral density (green b), and crosses the midline. These findings are consistent with a diagnosis of glioblastoma multiforme. Included in the differential diagnosis for lesions crossing the midline is primary lymphoma of the brain code
Image Courtesy Elisa Flower MD and Asim Mian MD 97644c.8
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
GBM in the Splenium
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
GBM in the Splenium
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Neonatal Corpus Callosum by Ultrasound
The ultrasound of a 7 day old baby boy reveals a normal sagittal section through the brain showing the CSF filled lateral ventricle (light blue) with most the brain substance showing characteristic homogeneous solid organ texture. The echogenic interfaces of the sulci with the gyri enable the outline of characteristic forms of the gyri so that for example the cingulate gyrus (darker green) is easily recognized by its classical location above the corpus callosum (purple). The corpus callosum is hypoechoic and overlaid in purple. The thalamus is isoechoic (orange) recognized by its position and shape rather than any unique ultrasound characteristics. The forebrain including the frontal parietal and temporal lobes are overlaid in green
Courtesy Ashley Davidoff MD Copyright 2010 90986c02.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Neonatal Corpus Callosum by Ultrasound
The ultrasound of a 7 day old baby boy reveals a normal sagittal section through the brain showing the CSF filled lateral ventricle (light blue) with most the brain substance showing characteristic homogeneous solid organ texture. The echogenic interfaces of the sulci with the gyri enable the outline of characteristic forms of the gyri so that for example the cingulate gyrus (darker green) is easily recognized by its classical location above the corpus callosum (purple). The corpus callosum is hypoechoic and overlaid in purple. The thalamus is isoechoic (orange) recognized by its position and shape rather than any unique ultrasound characteristics. The forebrain including the frontal parietal and temporal lobes are overlaid in green
Courtesy Ashley Davidoff MD Copyright 2010 90986c02.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The ultrasound of a 7 day old baby boy reveals a normal sagittal section through the brain showing the CSF filled lateral ventricle (light blue) with most the brain substance showing characteristic homogeneous solid organ texture. The echogenic interfaces of the sulci with the gyri enable the outline of characteristic forms of the gyri so that for example the cingulate gyrus (darker green) is easily recognized by its classical location above the corpus callosum (purple). The corpus callosum is hypoechoic and overlaid in purple. The thalamus is isoechoic (orange) recognized by its position and shape rather than any unique ultrasound characteristics. The forebrain including the frontal parietal and temporal lobes are overlaid in green
Courtesy Ashley Davidoff MD Copyright 2010 90986c02.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The ultrasound of a 7 day old baby boy reveals a normal sagittal section through the brain showing the CSF filled lateral ventricle (light blue) with most the brain substance showing characteristic homogeneous solid organ texture. The echogenic interfaces of the sulci with the gyri enable the outline of characteristic forms of the gyri so that for example the cingulate gyrus (darker green) is easily recognized by its classical location above the corpus callosum (purple). The corpus callosum is hypoechoic and overlaid in purple. The thalamus is isoechoic (orange) recognized by its position and shape rather than any unique ultrasound characteristics. The forebrain including the frontal parietal and temporal lobes are overlaid in green
Courtesy Ashley Davidoff MD Copyright 2010 90986c02.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Neonatal Corpus Callosum by Ultrasound
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Neonatal Corpus Callosum by Ultrasound
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Genu and Splenium at a Lower Level
The axial T2 weighted MRI is taken through the level of the ventricles. The body of the corpus callosum is above this level. The most anterior portion of the corpus callosum and most posterior portion are seen at this lower level of the ventricles
Courtesy Ashley Davidoff MD copyright 2010 all rights reserved 94079c04b05.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Genu and Splenium at a Lower Level
The axial T2 weighted MRI is taken through the level of the ventricles. The body of the corpus callosum is above this level. The most anterior portion of the corpus callosum and most posterior portion are seen at this lower level of the ventricles
Courtesy Ashley Davidoff MD copyright 2010 all rights reserved 94079c04b05.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The axial T2 weighted MRI is taken through the level of the ventricles. The body of the corpus callosum is above this level. The most anterior portion of the corpus callosum and most posterior portion are seen at this lower level of the ventricles
Courtesy Ashley Davidoff MD copyright 2010 all rights reserved 94079c04b05.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The axial T2 weighted MRI is taken through the level of the ventricles. The body of the corpus callosum is above this level. The most anterior portion of the corpus callosum and most posterior portion are seen at this lower level of the ventricles
Courtesy Ashley Davidoff MD copyright 2010 all rights reserved 94079c04b05.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Genu and Splenium at a Lower Level
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Genu and Splenium at a Lower Level
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
92170c03.8s
92170c03.8s The inversion recovery MRI sagittal section through the midline of the brain shows the forebrain superiorly and the corpus callosum (maroon) parralleling the course of the forebrain lying inferiorly code brain forebrain corpus callosum MRI inversion recovery proton density Images provided by Philips Medical Systems Modified and artictically rendered by Davidoff art copyright 2010 all rights reserved
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
92170c03.8s
92170c03.8s The inversion recovery MRI sagittal section through the midline of the brain shows the forebrain superiorly and the corpus callosum (maroon) parralleling the course of the forebrain lying inferiorly code brain forebrain corpus callosum MRI inversion recovery proton density Images provided by Philips Medical Systems Modified and artictically rendered by Davidoff art copyright 2010 all rights reserved
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 92170c03.8s The inversion recovery MRI sagittal section through the midline of the brain shows the forebrain superiorly and the corpus callosum (maroon) parralleling the course of the forebrain lying inferiorly code brain forebrain corpus callosum MRI inversion recovery proton density Images provided by Philips Medical Systems Modified and artictically rendered by Davidoff art copyright 2010 all rights reserved
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 92170c03.8s The inversion recovery MRI sagittal section through the midline of the brain shows the forebrain superiorly and the corpus callosum (maroon) parralleling the course of the forebrain lying inferiorly code brain forebrain corpus callosum MRI inversion recovery proton density Images provided by Philips Medical Systems Modified and artictically rendered by Davidoff art copyright 2010 all rights reserved
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
92170c03.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
92170c03.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Corpus Callosum
49079 Brain Normal Frontal lobe pariental lobe temporal lobe Cerebellum lateral ventricle fourth ventricle Pons Thalamus cerebral aqueduct genu corpus callosum 61 Male T1 sagital Courtesy Ashley Davidoff MD Uploaded RP
71431.800 brain cerebral anatomy corpus callosum third ventricle occipital lobe basilar artery pons cerebellum pons cerebellum normal MRI T2 weighted images
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Corpus Callosum
49079 Brain Normal Frontal lobe pariental lobe temporal lobe Cerebellum lateral ventricle fourth ventricle Pons Thalamus cerebral aqueduct genu corpus callosum 61 Male T1 sagital Courtesy Ashley Davidoff MD Uploaded RP
71431.800 brain cerebral anatomy corpus callosum third ventricle occipital lobe basilar artery pons cerebellum pons cerebellum normal MRI T2 weighted images
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 49079 Brain Normal Frontal lobe pariental lobe temporal lobe Cerebellum lateral ventricle fourth ventricle Pons Thalamus cerebral aqueduct genu corpus callosum 61 Male T1 sagital Courtesy Ashley Davidoff MD Uploaded RP
71431.800 brain cerebral anatomy corpus callosum third ventricle occipital lobe basilar artery pons cerebellum pons cerebellum normal MRI T2 weighted images
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 49079 Brain Normal Frontal lobe pariental lobe temporal lobe Cerebellum lateral ventricle fourth ventricle Pons Thalamus cerebral aqueduct genu corpus callosum 61 Male T1 sagital Courtesy Ashley Davidoff MD Uploaded RP
71431.800 brain cerebral anatomy corpus callosum third ventricle occipital lobe basilar artery pons cerebellum pons cerebellum normal MRI T2 weighted images
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Corpus Callosum
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Corpus Callosum
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Corpus Callosum 49079b05b03
49079b05b03 brain cerebrum cerebral corpus callosum normal anatomy MRI T1 weighted sagital Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Corpus Callosum 49079b05b03
49079b05b03 brain cerebrum cerebral corpus callosum normal anatomy MRI T1 weighted sagital Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 49079b05b03 brain cerebrum cerebral corpus callosum normal anatomy MRI T1 weighted sagital Davidoff MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 49079b05b03 brain cerebrum cerebral corpus callosum normal anatomy MRI T1 weighted sagital Davidoff MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Corpus Callosum 49079b05b03
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Corpus Callosum 49079b05b03
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Corpus Callosum – Distinctive Shape, Position and White Color
The midsagittal section view of brain reveals the distinctive shape position and character of the corpus callosum
The distinction between the character of the cerebral cortex which has a creamy color and the white matter exemplified by the corpus callosum (c) which is white, and the midbrain (mb) pons (p) and medulla (m) which are off white as opposed to the color of the cerebellum (c) which is light salmon pink is well demonstrated.
The relative sizes of the forebrain, midbrain and hindbrain are well appreciated in this section.
Image Courtesy of Thomas W.Smith, MD; Department of Pathology, University of Massachusetts Medical School. 97805b01
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Corpus Callosum – Distinctive Shape, Position and White Color
The midsagittal section view of brain reveals the distinctive shape position and character of the corpus callosum
The distinction between the character of the cerebral cortex which has a creamy color and the white matter exemplified by the corpus callosum (c) which is white, and the midbrain (mb) pons (p) and medulla (m) which are off white as opposed to the color of the cerebellum (c) which is light salmon pink is well demonstrated.
The relative sizes of the forebrain, midbrain and hindbrain are well appreciated in this section.
Image Courtesy of Thomas W.Smith, MD; Department of Pathology, University of Massachusetts Medical School. 97805b01
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 4
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The midsagittal section view of brain reveals the distinctive shape position and character of the corpus callosum
The distinction between the character of the cerebral cortex which has a creamy color and the white matter exemplified by the corpus callosum (c) which is white, and the midbrain (mb) pons (p) and medulla (m) which are off white as opposed to the color of the cerebellum (c) which is light salmon pink is well demonstrated.
The relative sizes of the forebrain, midbrain and hindbrain are well appreciated in this section.
Image Courtesy of Thomas W.Smith, MD; Department of Pathology, University of Massachusetts Medical School. 97805b01
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The midsagittal section view of brain reveals the distinctive shape position and character of the corpus callosum
The distinction between the character of the cerebral cortex which has a creamy color and the white matter exemplified by the corpus callosum (c) which is white, and the midbrain (mb) pons (p) and medulla (m) which are off white as opposed to the color of the cerebellum (c) which is light salmon pink is well demonstrated.
The relative sizes of the forebrain, midbrain and hindbrain are well appreciated in this section.
Image Courtesy of Thomas W.Smith, MD; Department of Pathology, University of Massachusetts Medical School. 97805b01
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Corpus Callosum – Distinctive Shape, Position and White Color
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Corpus Callosum – Distinctive Shape, Position and White Color
)
