Structure
The Common Vein Copyright 2007
Ashley Davidoff MD
Cristina Cesaro
Introduction
The
The unique structure of the aorta enables it to perform its essential function as a conduit for the transport of blood. The aorta?s relative location, size, shape, and composition, all work in concert to receive and transport blood as it is pumped out of the heart guiding blood into the systemic circulation.
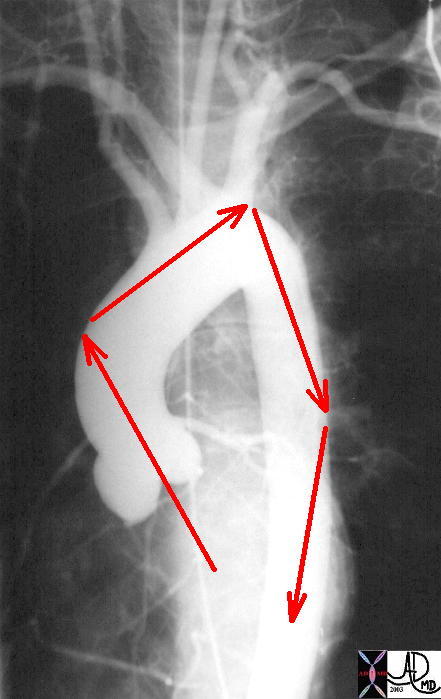
Direction of Blood Flow in the Ascendinhg Aorta and Arch
|
| This normal angiogram of the thoracic aorta shows the areas of shear stress on the aorta. The orientation of the ascending aorta is such that the jet of the LVejection is directed to the right lateral wall of the aorta. The second region of shear stress is just beyond the left subclavian artery, while the third is at the proximal thoracic aorta. The course thereafter is a straight shot to the bifurcation.
Courtesy Ashley Davidoff MD 27185 01 |
The aorta?s gross anatomy is sequentially divided into the ascending aorta, aortic arch, descending thoracic and abdominal aorta. Originating from the left ventricle, the aorta briefly arches above the plane of the heart. It then descends in the chest cavity, passes into the abdominal cavity through the diaphragm at the aortic hiatus, and terminates by bifurcating into the iliac arteries just above the pelvic cavity. Along its course, a series of arteries branch off, providing oxygenated blood to the heart, brain, upper limbs, airways, abdominal and pelvic cavities, and the legs. The largest branches arise from the top of the aortic arch. They include the brachiocephalic artery, the left common carotid and the left subclavian arteries.
The aorta is responsible for maintaining the pressure and velocity of the blood both of which are accomplished as a result of the contractile forces of the heart, the prevention of backflow by the aortic valves, and the control of flow by the peripheral arterioles called the precapillary sphincters. The contractile forces of the heart eject the blood via concentric contraction through the aortic valve. The aortic valve lies at the base of the heart and consists of three fibrous leaflets which work in concert to prevent backflow into the heart. The peripheral arterioles become muscular at the precapillary level and flow is controlled by neural hormonal and local factors depending on the end organ need. The conglomerate effect of the precapillary sphincters is to create a peripheral resistance.
In comparison with all the other arteries of the body, the aorta is by far the largest in diameter (approximately 3 cm at its origin). This trait allows the aorta to receive and transport a large volume of blood in order to efficiently supply the varied metabolic needs of each of the organs or structures. If minute arterioles replaced the aorta as the receptor of cardiac output there would be tremendous back flow into the left ventricle due to the tremendous resistance the ejecting volume would be faced with, not to mention an entirely incompatible system for maintaining proper pressure and flow.
The aorta?s wall is composed of layered muscular and elastic tissue. Stretching of the aorta provides the potential energy needed to propel the blood forward and maintain a high mean pressure sufficient to enable forward flow throughout diastole. The wall is divided into the tunica intima, media and adventitia. The tunica media comprises the majority of these elastic layers. Its discretely packaged fibers contribute greatly to the aorta?s distensible nature. Also, the tunica media, as well as the other layers, contributes to the aorta?s impressive radial strength. Such a property, accomplished by its unique makeup, helps mediate the rate of blood flow under high pressure conditions. Without such strong and flexible constituents, the aorta would simply be a large and rigid tube, unable to aid and adapt to oscillations in blood flow and pressure.
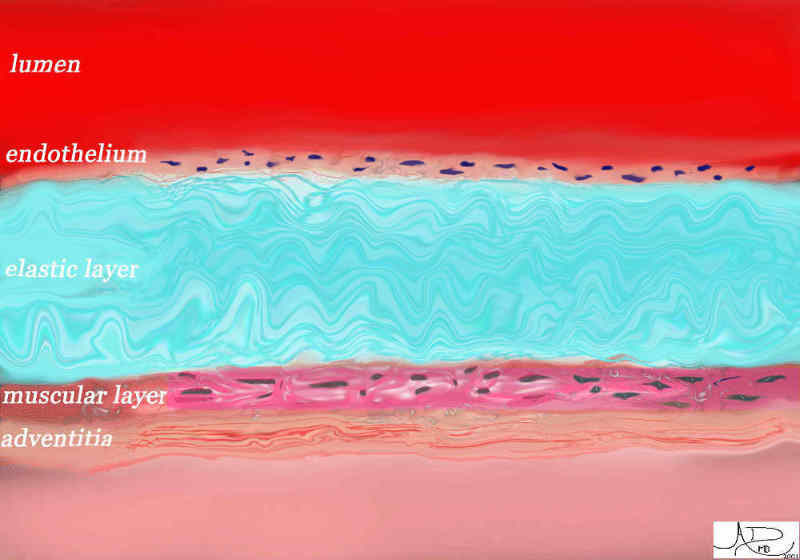
Histology – Key to Aortic Function is its Elastic Layer (teal)
The Innermost layer is the Endothelium and Outermost is the Adventitia |
| 47678.800 Davidoff art Davidof MD |
Applied Biology
Loss of elasticity is a normal result of aging and wear and tear of the aorta. Atherosclerosis is an aging process, and in general causes a decrease in elasticity, and compliance. It is usual and normal for the diameter of the aorta to enlarge by about 1mm per year starting in the 6th decade. Aneurysmal disease is an accelerated progression of the weakening of the aortic wall. In this entity the integrity of the aorta is challenged with progressive dilatation (about 2-3mms per year) and rupture becomes a significant risk and a life threatening situation. Surgical repair usually is indicated when aneurysms reach a critical size. Occlusive atherosclerotic disease is more common in the branches of the aorta though with severe atherosclerosis, occlusion of the distal abdominal aorta is possible. It is usually well tolerated because it is a slow process and adaptive collateral flow through the inferior mesenteric artery, lumbar and iliac arteries maintain blood flow to the lower extremities.
Congenital abnormalities are usually of a stenotic nature. Aortic valve stenosis due to a bicuspid aortic valve, when mild, is overcome by left ventricular hypertrophy. As stenosis progresses, compensatory mechanisms reach a limit with consequent heart failure and pulmonary congestion. Coarctation of the aorta is a congenital narrowing as well, usually occurring at the end of the arch in a segment of the aorta called the isthmus. Left ventricular hypertrophy results to overcome resistance created by the narrowing, while collateral channels develop to bypass the narrowing.
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Histology – Key to Aortic Function is its Elastic Layer (teal)
The Innermost layer is the Endothelium and Outermost is the Adventitia
47678.800 Davidoff art Davidof MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Histology – Key to Aortic Function is its Elastic Layer (teal)
The Innermost layer is the Endothelium and Outermost is the Adventitia
47678.800 Davidoff art Davidof MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => 47678.800 Davidoff art Davidof MD
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => 47678.800 Davidoff art Davidof MD
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Histology – Key to Aortic Function is its Elastic Layer (teal)
The Innermost layer is the Endothelium and Outermost is the Adventitia
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Histology – Key to Aortic Function is its Elastic Layer (teal)
The Innermost layer is the Endothelium and Outermost is the Adventitia
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Direction of Blood Flow in the Ascendinhg Aorta and Arch
This normal angiogram of the thoracic aorta shows the areas of shear stress on the aorta. The orientation of the ascending aorta is such that the jet of the LVejection is directed to the right lateral wall of the aorta. The second region of shear stress is just beyond the left subclavian artery, while the third is at the proximal thoracic aorta. The course thereafter is a straight shot to the bifurcation.
Courtesy Ashley Davidoff MD 27185 01
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Direction of Blood Flow in the Ascendinhg Aorta and Arch
This normal angiogram of the thoracic aorta shows the areas of shear stress on the aorta. The orientation of the ascending aorta is such that the jet of the LVejection is directed to the right lateral wall of the aorta. The second region of shear stress is just beyond the left subclavian artery, while the third is at the proximal thoracic aorta. The course thereafter is a straight shot to the bifurcation.
Courtesy Ashley Davidoff MD 27185 01
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This normal angiogram of the thoracic aorta shows the areas of shear stress on the aorta. The orientation of the ascending aorta is such that the jet of the LVejection is directed to the right lateral wall of the aorta. The second region of shear stress is just beyond the left subclavian artery, while the third is at the proximal thoracic aorta. The course thereafter is a straight shot to the bifurcation.
Courtesy Ashley Davidoff MD 27185 01
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This normal angiogram of the thoracic aorta shows the areas of shear stress on the aorta. The orientation of the ascending aorta is such that the jet of the LVejection is directed to the right lateral wall of the aorta. The second region of shear stress is just beyond the left subclavian artery, while the third is at the proximal thoracic aorta. The course thereafter is a straight shot to the bifurcation.
Courtesy Ashley Davidoff MD 27185 01
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Direction of Blood Flow in the Ascendinhg Aorta and Arch
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Direction of Blood Flow in the Ascendinhg Aorta and Arch
)
