
The Common Vein Copyright 2007
Ashley Davidoff MD
Approach
Since most cysts of the pancreas are in fact pseudocysts, and are related to alcoholic pancreatitis, the challenge is to identify the nature of a cyst when there is no history of alcohol abuse or prior alcoholic pancreatitis. The finding of solid components, thickened or enhancing septa and calcifications intimately associated with the cysts should caution against the diagnosis of a pseudocyst. The presence of an epithelial lining to the cyst make a tremendous difference to the biology of the cyst in both the clinical and radiological realms. Unfortunately when the epithelial surface is a simple single layer, we have no current ability to know this except by pathologic examination.
CT is the workhorse of the abdomen, but like in so many other instances it cannot adequately characterize fluid collections. We thus commonly depend on a multimodality approach for this entity.
Differential Diagnosis
Pseudocysts
acute pancreatitis
abdominal trauma
iatrogenic ? surgery
idiopathic
Retntion Cyst
Occur as a result of a blocked duct commonly caused in patients with a history of alcoholism and chronic pancreatitis where the ducts become inspissated with porteinacious precipitate, with secondary obstruction, dilatation and cyst formation. Thse cysts are usually in the 1-2cms range.
Neoplasm
Cystic neoplasms of the pancreas account for only 1% of primary pancreatic lesions.
serous cystadenoma
benign, female, tiny cysts, (but may be up to 2cms) large tumor, may be head body or tail, central stellate scar, +/- calcification
mucinous cystadenoma/ cystadenocarcinoma
benign, premalignant, or malignant, female++, large (mean 12cms) thick septations, 85% tail and body, scattered dystrophic calcifcation.
Rarer forms of cystic neoplasms of the pancreas include papillary cystic tumors, cystic islet cell tumor, acinar cystadenocarcinoma and lymphangioma.
Cystic neoplasms of the pancreas account for only 1% of primary pancreatic lesions.
serous cystadenoma
benign, female, tiny cysts, (but may be up to 2cms) large tumor, may be head body or tail, central stellate scar, +/- calcification. They rarely undergo malignant transformation
mucinous cystadenoma/ cystadenocarcinoma
benign, premalignant, or malignant, female++, large (mean 12cms) thick septations, 85% tail and body, scattered dystrophic calcification. Considered a mapremalignant process
Rarer forms of cystic neoplasms of the pancreas include papillary cystic tumors, cystic islet cell tumor, acinar cystadenocarcinoma and lymphangioma.
Congenital cysts
The congenital cysts are uncommon sometimes seen in autosomal dominant polycystic kidney disease and occasionally in patients with cystic fibrosis
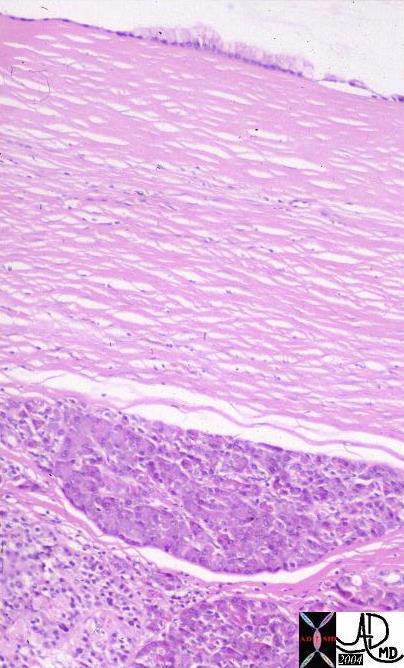 This histological section of the pancreas is from the records of a patient with a serous cystadenoma. The lumen of the cyst is at the top of the image and is cream colored. A single layer of epithelial cells lines the cyst. A pseudocyst on the other hand would have no epithelial lining.15316b01Courtesy Barbara Banner MD
This histological section of the pancreas is from the records of a patient with a serous cystadenoma. The lumen of the cyst is at the top of the image and is cream colored. A single layer of epithelial cells lines the cyst. A pseudocyst on the other hand would have no epithelial lining.15316b01Courtesy Barbara Banner MD
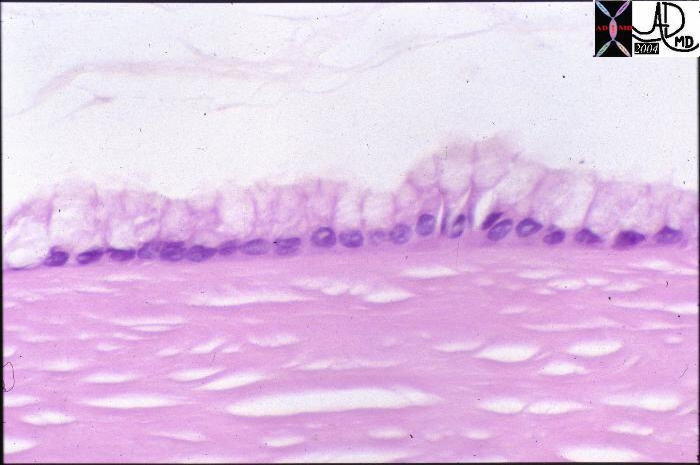 This high power view is of a histological section from the records of a patient with a serous cystadenoma of the pancreas. The lumen of the cyst is at the top of the image and is cream colored with floating debris. A single layer of columnar epithelial cells lines the cyst. A pseudocyst on the other hand would have no epithelial lining.15317 Courtesy Barbara Banner MD
This high power view is of a histological section from the records of a patient with a serous cystadenoma of the pancreas. The lumen of the cyst is at the top of the image and is cream colored with floating debris. A single layer of columnar epithelial cells lines the cyst. A pseudocyst on the other hand would have no epithelial lining.15317 Courtesy Barbara Banner MD
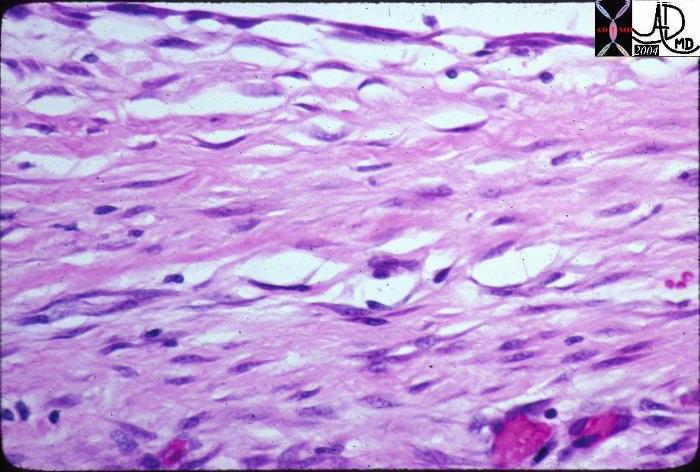 This high powered histological section is from the records of a patient with a pseudocyst. At the top of the image the white space represents the cyst lumen. The lining is made of fibrous tissue rather than an epithelium. A true cyst is lined by epithelial cells. 15306 Courtesy Barbara Banner MD
This high powered histological section is from the records of a patient with a pseudocyst. At the top of the image the white space represents the cyst lumen. The lining is made of fibrous tissue rather than an epithelium. A true cyst is lined by epithelial cells. 15306 Courtesy Barbara Banner MD
Pseudocysts
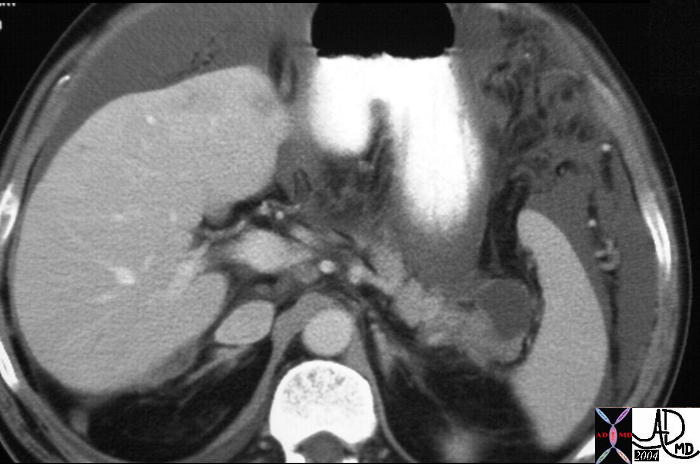
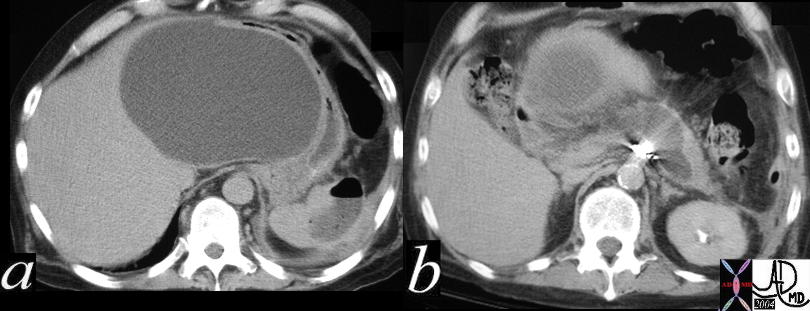 The CT scan of the abdomen shows a large cystic lesion in the lesser sac impinging on the medial aspect of the left lobe of the liver and the medial aspect of the stomach. The cyst is seen to arise from the head of the pancreas and extends into the body. An abscess with an air fluid level is identified in the spleen in a, while spray artifact is noted in the second image. The findings are consistent with a large pseudocyst secondary to acute alcoholic pancreatitis. The pancreatitis was also complicated by a pseudoaneurysm which was treated by coil embolization (spray artifact) and a splenic abscess. 40117c Courtesy Ashley Davidoff MD
The CT scan of the abdomen shows a large cystic lesion in the lesser sac impinging on the medial aspect of the left lobe of the liver and the medial aspect of the stomach. The cyst is seen to arise from the head of the pancreas and extends into the body. An abscess with an air fluid level is identified in the spleen in a, while spray artifact is noted in the second image. The findings are consistent with a large pseudocyst secondary to acute alcoholic pancreatitis. The pancreatitis was also complicated by a pseudoaneurysm which was treated by coil embolization (spray artifact) and a splenic abscess. 40117c Courtesy Ashley Davidoff MD
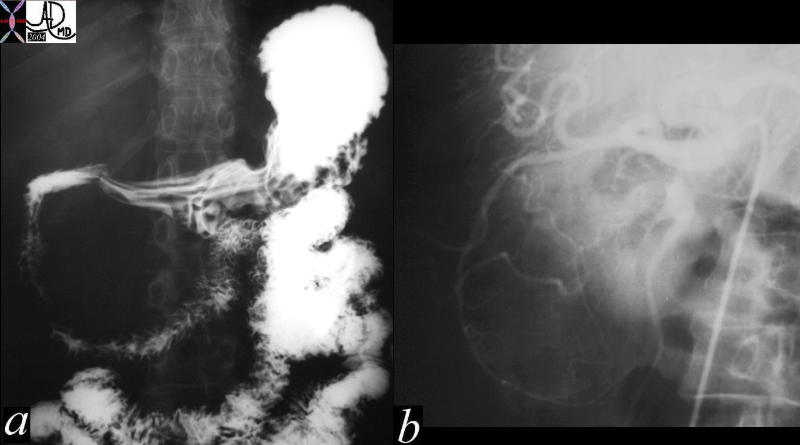 This GI study and angiogram is from a 49 year old female who was two years post cholecystectomy and presented with weight loss and increasing mass on the right side of her abdomen. The upper GI study shows widening of the C sweep of the duodenum and the angiogram shows splaying of the gastroduodenal artery around a large smooth, and avascular mass. These findings are consistent with a pseudocyst of the pancreas. At surgery a large pseudocyst was found and cyst gastrostomy was performed. 40893c Courtesy Laura Feldman MD
This GI study and angiogram is from a 49 year old female who was two years post cholecystectomy and presented with weight loss and increasing mass on the right side of her abdomen. The upper GI study shows widening of the C sweep of the duodenum and the angiogram shows splaying of the gastroduodenal artery around a large smooth, and avascular mass. These findings are consistent with a pseudocyst of the pancreas. At surgery a large pseudocyst was found and cyst gastrostomy was performed. 40893c Courtesy Laura Feldman MD
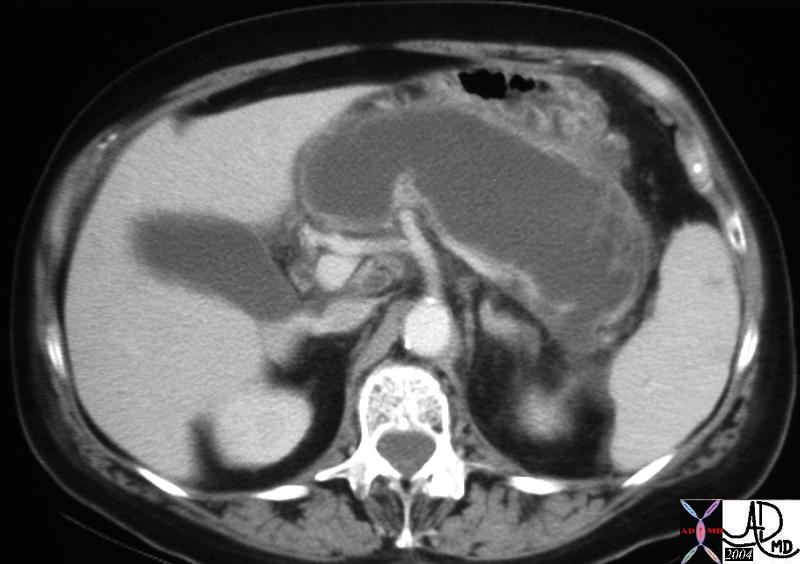
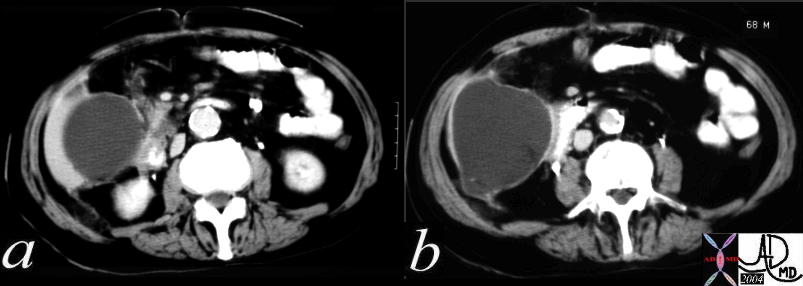 The CT scan is of a 68 year old male with epigastric pain and shows a large cystic lesion at the inferior aspect of the liver. The anatomical differential for this lesion included the gallbladder, the liver itself, or the pancreas. In this case it represented a pseudocyst of the pancreas. 40219c01 Courtesy Ashley Davidoff MD
The CT scan is of a 68 year old male with epigastric pain and shows a large cystic lesion at the inferior aspect of the liver. The anatomical differential for this lesion included the gallbladder, the liver itself, or the pancreas. In this case it represented a pseudocyst of the pancreas. 40219c01 Courtesy Ashley Davidoff MD
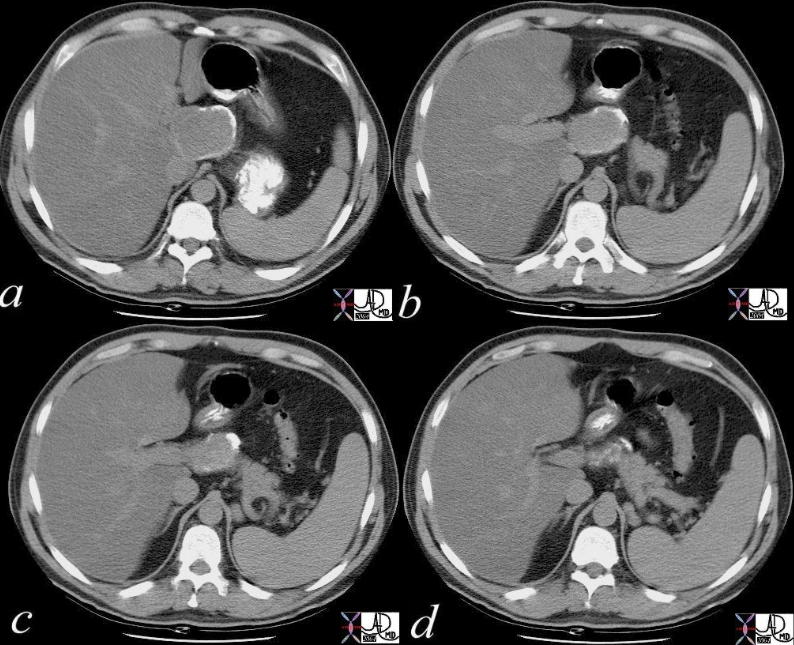
 The CT scan is from an elderly man with a mass in the head of the pancreas who underwent an intraoperative pancreatic biopsy, and who subsequently presented with abdominal pain and a left groin mass. The cystic lesion of the pancreas extends to the left paracolic gutter (b), and then to the left paraortic position and iliacus (c), and finally along the iliopsoas muscle (d). Note the thickening of the involved descending colon. (c). The findings are consistent with a pseudocyst of iatrogenic trauma that dissected from the pancreas to the left groin. 40242c Courtesy Ashley Davidoff MD
The CT scan is from an elderly man with a mass in the head of the pancreas who underwent an intraoperative pancreatic biopsy, and who subsequently presented with abdominal pain and a left groin mass. The cystic lesion of the pancreas extends to the left paracolic gutter (b), and then to the left paraortic position and iliacus (c), and finally along the iliopsoas muscle (d). Note the thickening of the involved descending colon. (c). The findings are consistent with a pseudocyst of iatrogenic trauma that dissected from the pancreas to the left groin. 40242c Courtesy Ashley Davidoff MD
 This CTscan through the pancreas shows a cystic mass in the pancreatic tail associated with surgical absence of the left kidney, a left adrenal nodule and a cholesterol gall stone. Prior surgery with iatrogenic trauma to the tail of the pancreas is the most likely cause of the pseudocyst. The cystic nature needs to be verified by US. 25055 Courtesy Ashley Davidoff MD
This CTscan through the pancreas shows a cystic mass in the pancreatic tail associated with surgical absence of the left kidney, a left adrenal nodule and a cholesterol gall stone. Prior surgery with iatrogenic trauma to the tail of the pancreas is the most likely cause of the pseudocyst. The cystic nature needs to be verified by US. 25055 Courtesy Ashley Davidoff MD
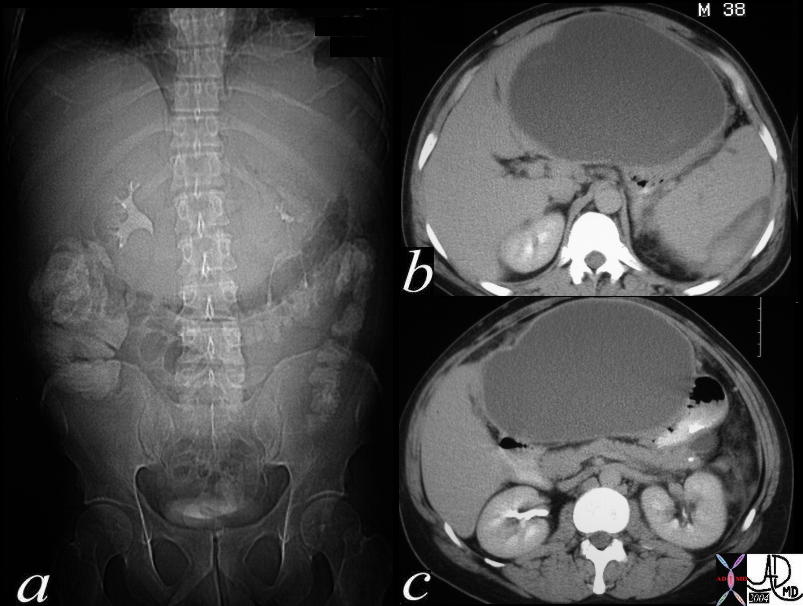 This CTscan is of a 38 year old male with abdominal distension. The scout study shows inferior displacement of the transverse colon by a large epigastric mass. A large cystic structure impinging on the medial left lobe of the liver and the medial aspect of the stomach suggest a pseudocyst arising in the lesser sac from the pancreas and a diagnosis of a pancreatic pseudocyst secondary to acute alcoholic pancreatitis is most likely. The high density material around the spleen in b represents a subcapsular splenic hematoma. 40283c Courtesy Ashley Davidoff MD
This CTscan is of a 38 year old male with abdominal distension. The scout study shows inferior displacement of the transverse colon by a large epigastric mass. A large cystic structure impinging on the medial left lobe of the liver and the medial aspect of the stomach suggest a pseudocyst arising in the lesser sac from the pancreas and a diagnosis of a pancreatic pseudocyst secondary to acute alcoholic pancreatitis is most likely. The high density material around the spleen in b represents a subcapsular splenic hematoma. 40283c Courtesy Ashley Davidoff MD
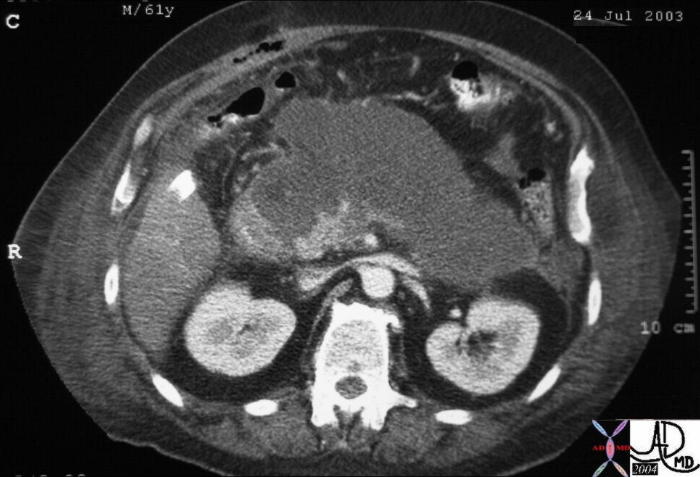
The CT scan of the abdomen of a 61 year old male shows a large cystic type lesion in the lesser sac, conforming to the shape of the pancreas. Note also the piecemeal appearance of the remaining viable pancreas in the region of the uncinate process. There was little other viable pancreas identified and a diagnosis of pancreatic necrosis was made. Associated findings include extension of the inflammatory process to the left paracolic gutter and through to the soft tissues of the flanks, as well as postoperative air in the right rectus abdominis muscle. 31188b01 Courtesy Ashley Davidoff MD
Chronic pseudocyst
 The CT scan of the abdomen shows a rim calcification of an exophytic mass that arises from the head of the pancreas. This finding represents a rim calcification of a pseudocyst of the pancreas. Calcification of this manner is unusual for pseudocysts. 17270c Courtesy Ashley Davidoff MD
The CT scan of the abdomen shows a rim calcification of an exophytic mass that arises from the head of the pancreas. This finding represents a rim calcification of a pseudocyst of the pancreas. Calcification of this manner is unusual for pseudocysts. 17270c Courtesy Ashley Davidoff MD
Neoplasm
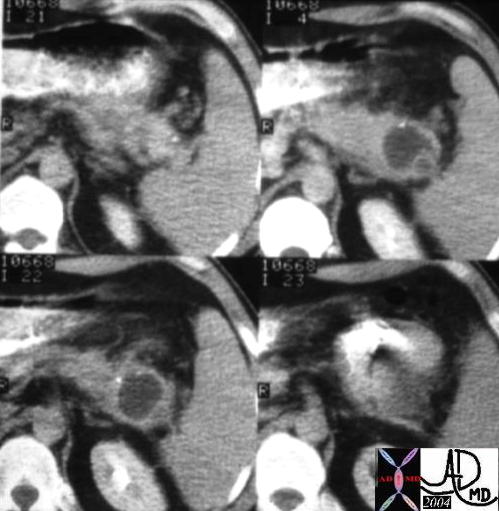 The CTscan through the body of the pancreas is of a 74 year old female with abdominal discomfort. She has no history of alcohol abuse and a normal US of the gallbladder. The study shows a complex, bilocular, cystic lesion in the tail of the pancreas with an enhancing rind, and two focal peripheral punctate calcifications. A diagnosis of a mucinous cystadenoma is thought to be most likely. 04811 Courtesy Ashley Davidoff MD
The CTscan through the body of the pancreas is of a 74 year old female with abdominal discomfort. She has no history of alcohol abuse and a normal US of the gallbladder. The study shows a complex, bilocular, cystic lesion in the tail of the pancreas with an enhancing rind, and two focal peripheral punctate calcifications. A diagnosis of a mucinous cystadenoma is thought to be most likely. 04811 Courtesy Ashley Davidoff MD
 The CTscan through the head of the pancreas is of a 75 year old female with abdominal discomfort. There is a multiloculated cystic mass in the head of the pancreas. The age sex, appearance, and location make a serous cystadenoma most likely. 40585 Courtesy Ashley Davidoff MD
The CTscan through the head of the pancreas is of a 75 year old female with abdominal discomfort. There is a multiloculated cystic mass in the head of the pancreas. The age sex, appearance, and location make a serous cystadenoma most likely. 40585 Courtesy Ashley Davidoff MD
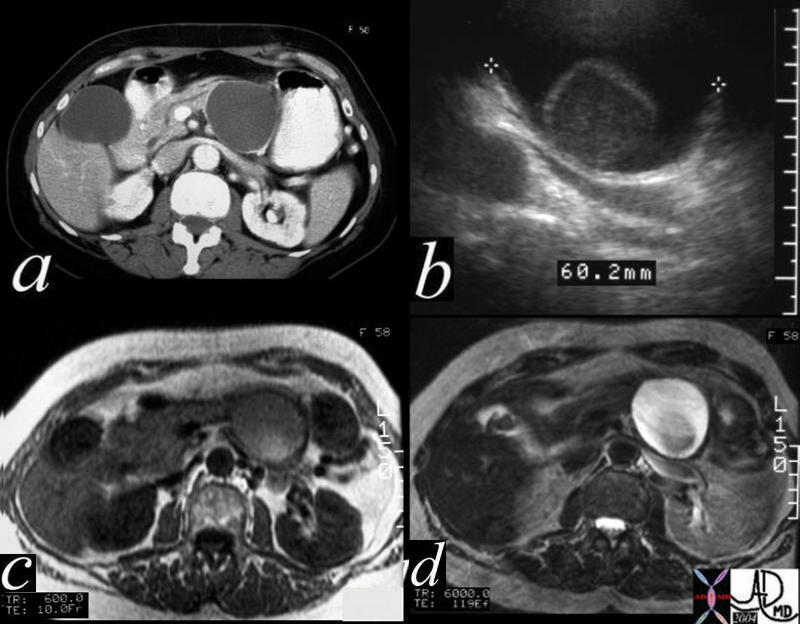 This CTscan is through the tail of the pancreas shows what appears to be a simple cyst (a), but which proves to have a mural nodule on ultrasound (b). On the T1 weighted image (c) the nodule shows high intensity suggesting increased protein or acute blood, and the T2 (d) reveals the cystic nature of the matrix. At pathology the lesion was a benign serous cystadenoma. The high intensity on T1 was due to the high protein in the mucin. 40487c01 Courtesy Ashley Davidoff MD
This CTscan is through the tail of the pancreas shows what appears to be a simple cyst (a), but which proves to have a mural nodule on ultrasound (b). On the T1 weighted image (c) the nodule shows high intensity suggesting increased protein or acute blood, and the T2 (d) reveals the cystic nature of the matrix. At pathology the lesion was a benign serous cystadenoma. The high intensity on T1 was due to the high protein in the mucin. 40487c01 Courtesy Ashley Davidoff MD
Malignant neoplasm
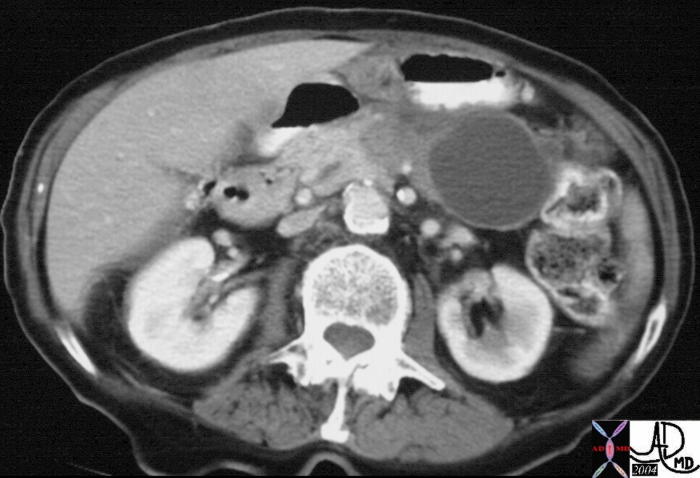 This CTscan of an 83 year old female is through the body and tail of the pancreas shows a complex cystic mass that has a cystic component with a thickened wall and a solid component medially that has a focal calcification. These findings are consistent with a mucinous cystadenocarcinoma which was pathologically proven. 19907 Courtesy Ashley Davidoff MD
This CTscan of an 83 year old female is through the body and tail of the pancreas shows a complex cystic mass that has a cystic component with a thickened wall and a solid component medially that has a focal calcification. These findings are consistent with a mucinous cystadenocarcinoma which was pathologically proven. 19907 Courtesy Ashley Davidoff MD
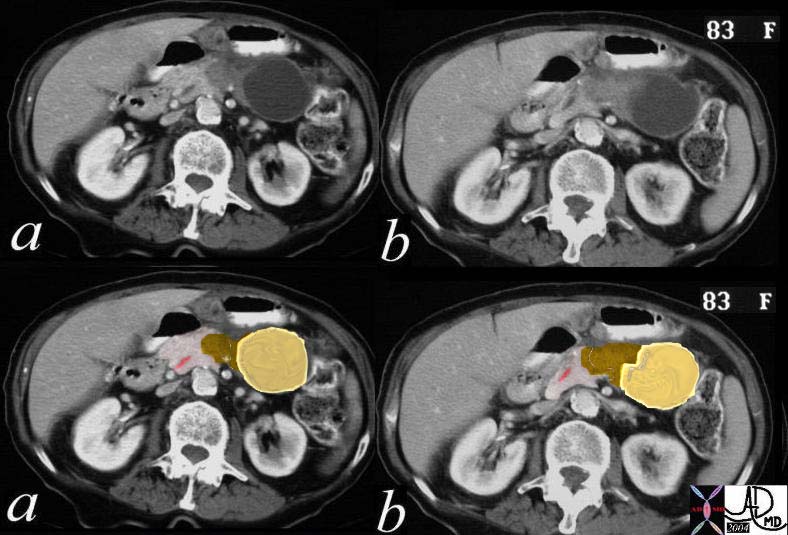 This CTscan of an 83 year old female is through the body and tail of the pancreas shows the complex cystic mass (a,b). In c and d, the cystic component with a thickened wall is shown in yellow, and the solid component medially with a focal calcification is shown in brown. The pancreatic duct which is minimally prominent is shown in pink. These findings are consistent with a mucinous cystadenocarcinoma which was pathologically proven. 19911c01b03 Courtesy Ashley Davidoff MD
This CTscan of an 83 year old female is through the body and tail of the pancreas shows the complex cystic mass (a,b). In c and d, the cystic component with a thickened wall is shown in yellow, and the solid component medially with a focal calcification is shown in brown. The pancreatic duct which is minimally prominent is shown in pink. These findings are consistent with a mucinous cystadenocarcinoma which was pathologically proven. 19911c01b03 Courtesy Ashley Davidoff MD
 This CT scan through the pancreas shows a complex cystic mass with dense, curvilinear peripheral dystrophic calcification in the tail of the pancreas. Associated findings include portal vein thrombosis (PVT) and ascites. These findings are consistent with a mucinous cystadenoma, and a malignant transformation of a mucinous neoplasm has to be considered in view of the PVT. An expanded version of this case appears below. 40712 Courtesy Ashley Davidoff MD
This CT scan through the pancreas shows a complex cystic mass with dense, curvilinear peripheral dystrophic calcification in the tail of the pancreas. Associated findings include portal vein thrombosis (PVT) and ascites. These findings are consistent with a mucinous cystadenoma, and a malignant transformation of a mucinous neoplasm has to be considered in view of the PVT. An expanded version of this case appears below. 40712 Courtesy Ashley Davidoff MD
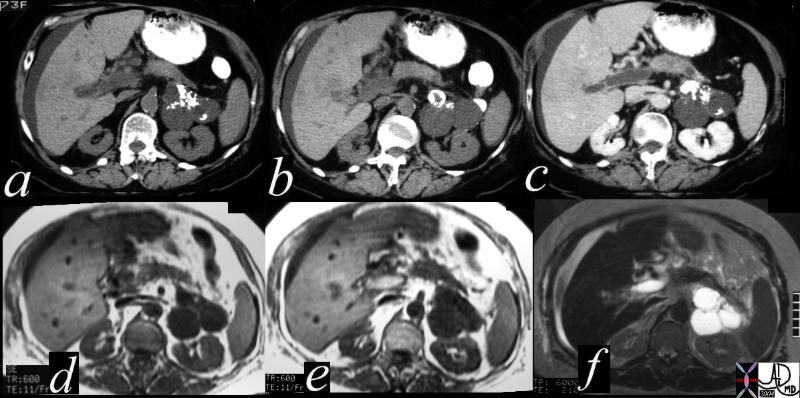 This CT scan through the pancreas (a,b,c) shows a complex cystic mass with dense peripheral dystrophic calcification in the tail of the pancreas. Associated findings include portal vein thrombosis (PVT) and ascites. The lesions on the T1 weighted image (d) are dark, and are bright on the T2 weighted image consistent with their cystic nature. The portal vein is bright on the T1 image and bright on T2 consistent with acute thrombus. These findings are consistent with a diagnosis of mucinous cystadenoma, and a malignant transformation of a mucinous neoplasm has to be considered in view of the PVT. 40717c Courtesy Ashley Davidoff MD
This CT scan through the pancreas (a,b,c) shows a complex cystic mass with dense peripheral dystrophic calcification in the tail of the pancreas. Associated findings include portal vein thrombosis (PVT) and ascites. The lesions on the T1 weighted image (d) are dark, and are bright on the T2 weighted image consistent with their cystic nature. The portal vein is bright on the T1 image and bright on T2 consistent with acute thrombus. These findings are consistent with a diagnosis of mucinous cystadenoma, and a malignant transformation of a mucinous neoplasm has to be considered in view of the PVT. 40717c Courtesy Ashley Davidoff MD
 This CT scan through the head of the pancreas shows a complex cystic mass with dense and thickened components best seen in the bottom right image. The lesion was biopsied and shown to be a cystadenocarcinoma. 40495c Courtesy Ashley Davidoff MD
This CT scan through the head of the pancreas shows a complex cystic mass with dense and thickened components best seen in the bottom right image. The lesion was biopsied and shown to be a cystadenocarcinoma. 40495c Courtesy Ashley Davidoff MD
 This CTscan through the head of the pancreas shows a small complex and heterogeneous mass, with dominant hypodensity. The anatomic differential diagnosis lies between the duct and the parenchyma. An ERCP was performed 18143 Courtesy Ashley Davidoff MD
This CTscan through the head of the pancreas shows a small complex and heterogeneous mass, with dominant hypodensity. The anatomic differential diagnosis lies between the duct and the parenchyma. An ERCP was performed 18143 Courtesy Ashley Davidoff MD
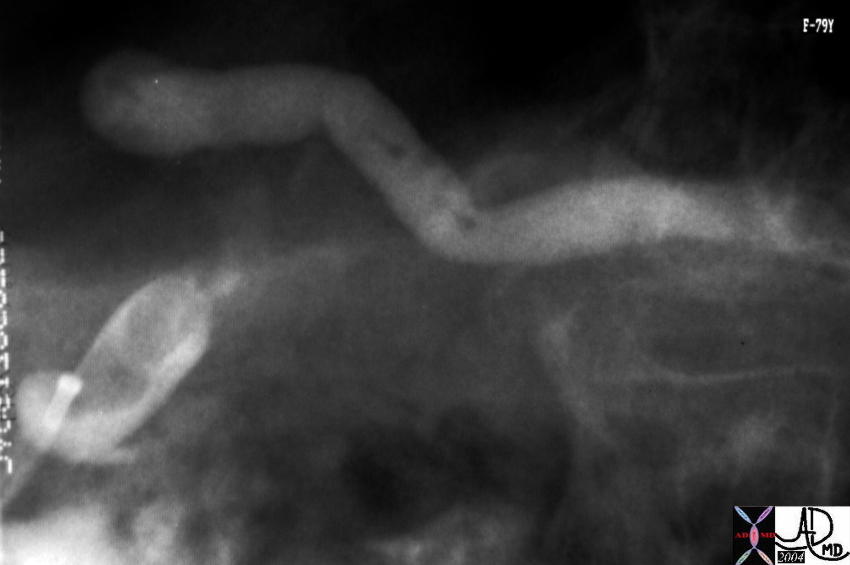 At ERCP mucoid material was noted in the ampulla. The lesion identified in the uncinate process on the CT was noted as a nodule in the duct. Associated findings included tubular thin filling defects in the duct of the body consistent with mucus. A diagnosis of mucinous duct ectasia with a papillary tumor with papillary and mucinous features was made at pathology. 40377 Courtesy Ashley Davidoff MD
At ERCP mucoid material was noted in the ampulla. The lesion identified in the uncinate process on the CT was noted as a nodule in the duct. Associated findings included tubular thin filling defects in the duct of the body consistent with mucus. A diagnosis of mucinous duct ectasia with a papillary tumor with papillary and mucinous features was made at pathology. 40377 Courtesy Ashley Davidoff MD
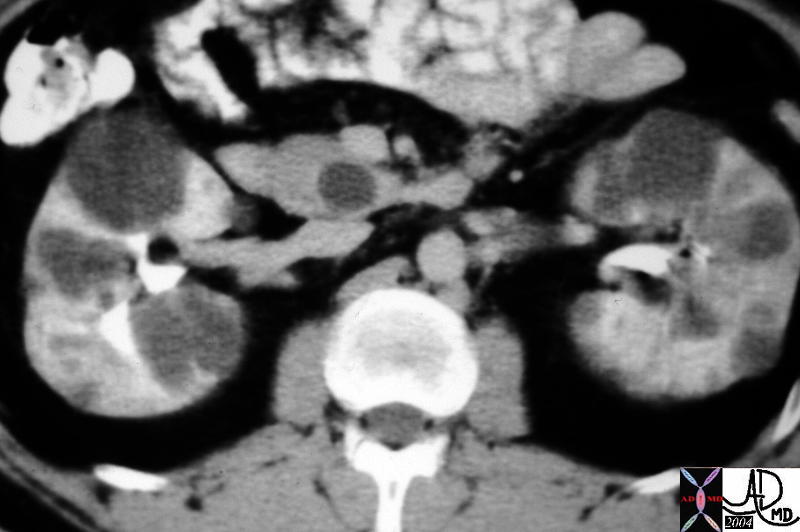
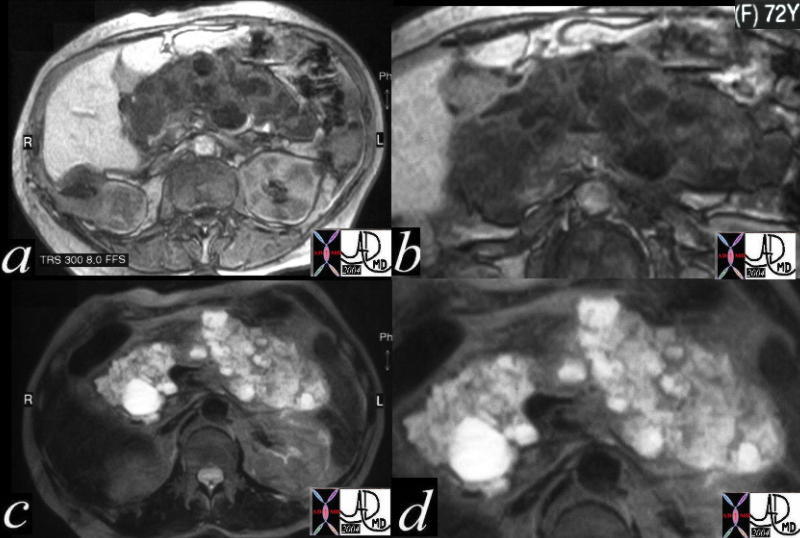 This CT scan in a 72 year old female through the pancreas shows a series of complex cystic and solid masses diffusely throughout the pancreas, with a few cystic masses in the right kidney. These findings are consistent with a diagnosis of von Hippel-Lindau syndrome in which the gamut of cystic and solid, benign and malignant tumors of the pancreas manifest. The benign lesions are usually serous cystadenomas. Mucinous tumors do not usually occur in the von Hippel-Lindau setting. 24061c Courtesy Ashley Davidoff MD
This CT scan in a 72 year old female through the pancreas shows a series of complex cystic and solid masses diffusely throughout the pancreas, with a few cystic masses in the right kidney. These findings are consistent with a diagnosis of von Hippel-Lindau syndrome in which the gamut of cystic and solid, benign and malignant tumors of the pancreas manifest. The benign lesions are usually serous cystadenomas. Mucinous tumors do not usually occur in the von Hippel-Lindau setting. 24061c Courtesy Ashley Davidoff MD
 This CT scan through the pancreas shows a cystic mass in the pancreatic tail associated with thickened gastrolienal ligament and ascites. This case represents transperitoneal spread of a known pancreatic carcinoma. Metastatic nodules are also noted in the liver. 20114 Courtesy Ashley Davidoff MD
This CT scan through the pancreas shows a cystic mass in the pancreatic tail associated with thickened gastrolienal ligament and ascites. This case represents transperitoneal spread of a known pancreatic carcinoma. Metastatic nodules are also noted in the liver. 20114 Courtesy Ashley Davidoff MD
Masqueraders
 This CTscan through the pancreas shows a tubular cystic mass in the pancreatic body and tail, which conforms to the shape of the pancreatic tail and is associated with a thin rim of pancreatic tissue. The finding is consistent with an obstructed and dilated pancreatic duct with secondary pressure atrophy of the pancreas. The focal hypodensity in the spleen is of unknown significance. 40208 Courtesy Ashley Davidoff MD
This CTscan through the pancreas shows a tubular cystic mass in the pancreatic body and tail, which conforms to the shape of the pancreatic tail and is associated with a thin rim of pancreatic tissue. The finding is consistent with an obstructed and dilated pancreatic duct with secondary pressure atrophy of the pancreas. The focal hypodensity in the spleen is of unknown significance. 40208 Courtesy Ashley Davidoff MD
 The CTscan through the head of the pancreas shows a punctate calcification in the region of the head of the pancreas in close contact with the cystic appearing CBD. Associated findings include induration around the head of the pancreas and thickening of the left sided Gerota?s fascia. These findings are consistent with a diagnosis of gallstone pancreatitis. 16225b03 Courtesy Ashley Davidoff MD
The CTscan through the head of the pancreas shows a punctate calcification in the region of the head of the pancreas in close contact with the cystic appearing CBD. Associated findings include induration around the head of the pancreas and thickening of the left sided Gerota?s fascia. These findings are consistent with a diagnosis of gallstone pancreatitis. 16225b03 Courtesy Ashley Davidoff MD