Laura Miller MD and Ashley Davidoff MD
The Common Vein
Copyright 2010
Definition
Uterine fibroids (leiomyomas) are benign tumors of the myometrium and are the most common female reproductive tract tumor. They occur in women of reproductive age.
Fibroids are caused by clonal proliferation of a single smooth muscle cell in response to estrogen and progesterone. Because their growth is hormone-responsive, they typically regress with menopause.
The structural changes are characterized by single or multiple masses of smooth muscle cells, with some fibrous tissue, within the myometrium. The masses may protrude into the uterine or abdominal cavities. Fibroids vary greatly in size and rarely may grow large enough to fill the abdomen and compress the abdominal organs.
The functional changes are variable, and depend on fibroid location and size. For many women the functional change is minimal. However, fibroids that project into the uterine cavity and distend the endometrium may cause increased menstrual bleeding as well as infertility.
Clinically many women with fibroids are asymptomatic and present clinically with incidental findings on imaging. However, women with multiple or larger fibroids may present with menorrhagia, pelvic pain, infertility or an irregular abdominal mass. Fibroids that outgrow their blood supply can undergo infarction and necrosis causing sudden severe pain.
Imaging evaluation of fibroids is usually done with ultrasound. MRI is useful in evaluation if ultrasound is non-diagnostic.
Diagnosis is made with findings on physical exam and imaging.
Treatment is variable depending on size and symptoms. Asymptomatic women with small fibroids can be managed with observation. Fibroids causing pain or infertility can be removed with laparoscopic or open myometomy. The blood supply of large individual fibroids can be targeted with uterine artery embolization. Women with large or symptomatic fibroids who have finished childbearing may be treated with hysterectomy.

Large and Lobular Uterus |
|
The CTscan is from a 31year old female, who presents with a pelvic mass.The study reveals a large uterus with multicentric fibroids and mild hydronephrosis The heterogeneous and lobular mass measures 17cms (c-c)by 10cms (A-P) by 12cms (transverse), and is consistent with a fibroid uterus.
Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 84362c.8s
|
|
Deformity of the Endometrial CAvity Caused by an Intramural Fibroid |
|
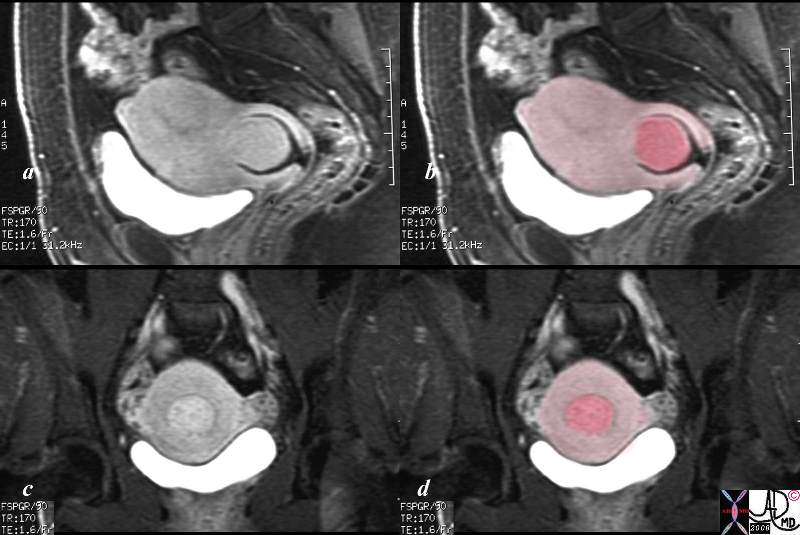
In this sagittal view of the T1 weighted contrast enhanced study of the the uterus of a 46 year old female. The uterus roughly retains its pear shaped structure but the shape of the endometrial cavity is distinctly abnormal as if there is something pushing on it from above. This patient has a diffusely enhancing isointense leiomyoma that impinges on the endometrial cavity.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 96577.8s
|
|

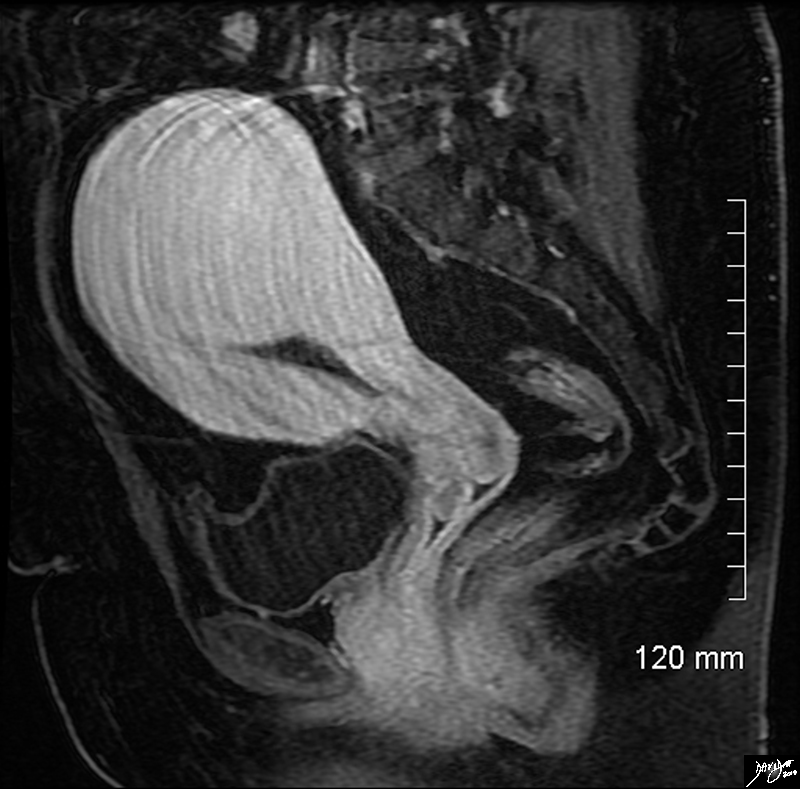
Large Intramural Fibroid Deforming the Stripe
T2 Weighted Image |
|
In this sagittal view of the T2 weighted MRI of the uterus of a 46 year old female an almost 6cms slightly hyperintense fibroid is seen pushing on the endometrial cavity from above. This patient has a large fibroid aka leiomyoma that impinges on the endometrial cavity.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 96570.8s
|
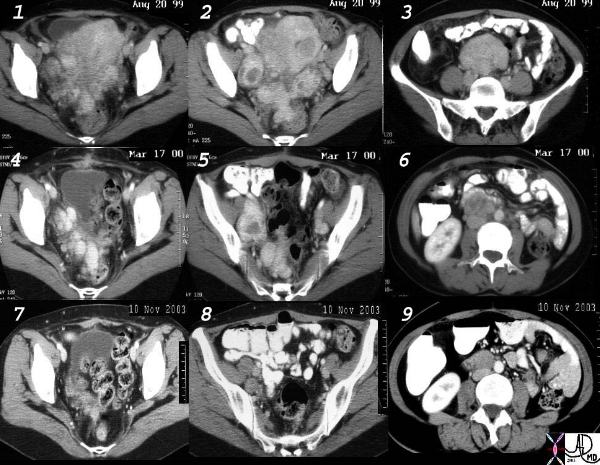
Benign Systemic Leiomyomatosis
|
|
This is a collage of CT findings of benign systemic leiomyomatosis over a 4 and half year period. Images 1,2,3 are from April 20th 1999 when the patient presented wth a pelvic mass with extensive hyperemic fibroid disease. Following hysterectomy a repeat CT of March 17 2000 shows residual disease in the pelvis, right internal iliac, and left internal iliac nodes (4,5,6). By November 2003 there was loss of the hyperemia and significant reduction of the tumor bulk. The patient was aged 47 at this time with a history of hepatitis being treated with interferon.
Courtesy Ashley Davidoff MD. – 32481c01
|
|
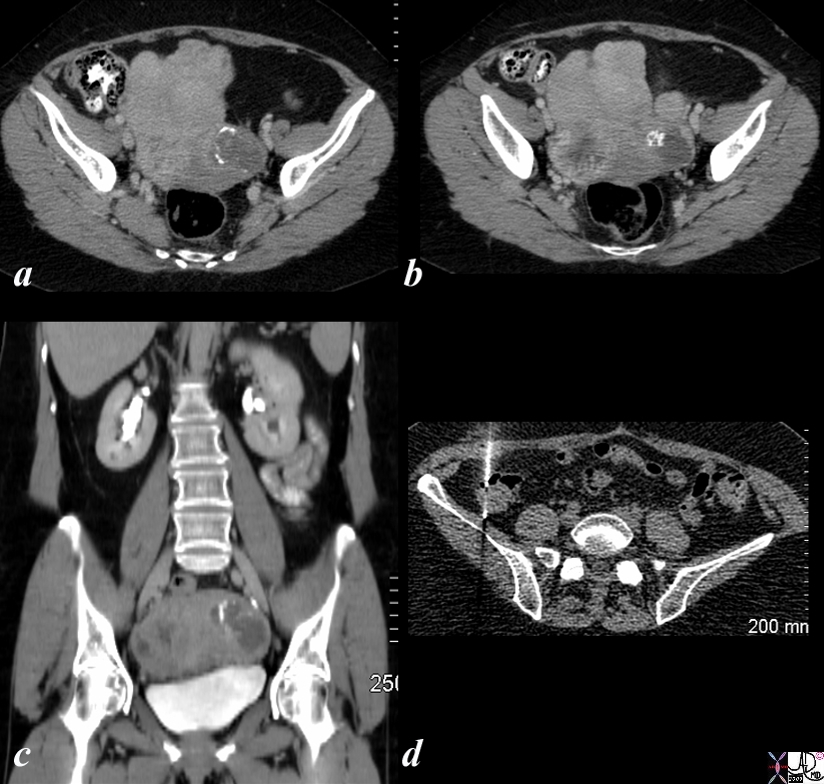
Leiomyosarcoma |
|
The CT is from a 58 year old post menopausal female who presents with an enlarging pelvic mass (a,b,c). CTscan shows multiple large masses in the uterus some of which are calcified consistent with leiomyomas. However clinically the mass had grown significantly in the last few months. Surgery revealed a leiomyosarcoma. Follow up CT 1 year later showed paracolic nodules which were proven to be metastatic deposits by biopsy (d).
Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 85519cL.8s
|
Uterine fibroids (leiomyomas) are benign tumors of the myometrium and are the most common female reproductive tract tumor. They are thought to arise from a single cell (? chromosomal aberration) and growth is affected by estrogen and progesterone. They typically regress with menopause.
These are very common benign tumors.
25% females suffer from fibroid disease, though 50% African American. In patients over 40 years, the incidence increases to 40%.
Types
Intramyometrial
Submucosal fibroids that have 50% or more imposition on the lumen can be removed hysteroscopically
Exophytic
More frequently they are asymptomatic and found incidentally on imaging. Symptoms attributed to fibroids are menorrhagia, pelvic pain, infertility and uterine incontinence or it can present as large abdominal masses. Management options are many and are guides by symptoms, age and reproductive status of the patient. This may include observation open or laproscopic myomectomy , uterine artery embolization and hysterectomy
They occupy space and in so doing may displace or obstruct other structures. They may cause pain during the menses and if they degenerate with disruption of their blood supply, sudden severe pelvic pain can occur. If a pedunculated fibroid becomes twisted on itself (torsion), this can cause acute pain.
Symptoms associated with these space occupying lesions can include irregular or prolonged menstrual bleeding, painful intercourse, and pressure on other structures located nearby including the bladder (urinary frequency) or bowels (constipation.)
Imaging
Vary in size from a few centimetres to as large as 20-30cms, most commonly intramyometrial, but can be submucosal or subserosal .
Ultrasound is the study of choice, but soemtimes the lesions are isodense and are difficult to visualize. They are usually of variable echogenicity and have poor through transmission
They are best and most consistently visualized with MRI, where they appear with intermediate or low signal on T1 and low signal on T2
When they degenerate they become heterogeneous as a result of cystic or hemorrhagic changes of varying age.
CT is not commonly used as a primary modality for diagnosis and characterization, but calcifications are best seen as ring-like or popcorn like in appearance. The enhancement pattern is also variable.
Sensitive to estrogen
Calcification is ring like or popcorn only in 10%
Margin is pushing not infiltrating
Degeneration
Few types
Hyaline – most common low attenuation on CT
High on T2
Cystic or myxoid degeneration occurs with progressive hyaline degeneration
Carneous or red degeneration = massive hemorrhagic infarction due to obstruction of veins = coagualitive necrosis and is seen with pregnancy
Fatty degeneration seen with lipoleiomyomas
Sarcomatous degeneration is rare <1% seen in postmenopausal females STUMP = smooth muscle tumors of uncertain malignant potential 1/3 of sarcomas of the uterus arise from a leiomyoma
Treatmentdepends on the clinical scenario, but usually for the pain syndromes it is symptomatic. Frequently, fibroids are incidental findings which can be managed expectantly. If there is significant pain suggestive of necrosis, bleeding, or infertility, surgery may be considered. Options include myomectomy (removal of the tumor only) or complete hysterectomy. In the appropriate clinical setting laparoscopic surgery is becoming the procedure of choice.
Sometimes, selective emboliziation is used, particulalrly when the fibroids are large. this is a percutaneous technique that involves selective catheterization of the feeding arteries and causing ischemia and infarction of the tumor. This usually results in a about a 50% reduction in the size of the fibroid.Submucosal fibroids that have 50% or more imposition on the lumen can be removed hysteroscopically
Other treatments include GnRH hypoestrogenism which cannot be given long term as it causes osteoporosis.
|
Submucosal Fibroid
|
| The USscan (sonohysterogram) scan is from a 41year old female, who presents with dysfunctional uterine bleeding. The study reveals a 4mms submucosal nodule shown at pathology to be a submucosal fibroid.
uterus fibroid leiomyoma submucosal USscan sonohysterogram Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 84299c041.8 |
|
Prolapsing Submucosal Fibroid
|
| This patient presented to the emergency room with severe crampy abdominal pain and a known history of a submucosal fibroid. The MRI shows the fibroid (dark pink) orotruding and expanding the cervix in the sagital view, and in the coronal view it is seen as a hyperemic structure (c) surrounded by lighter pink myometrium.
pain uterus submucosal fibroid prolapse MRI Courtesy Ashley DAvidoff MD copyright 2008 16265c01.8s |
|
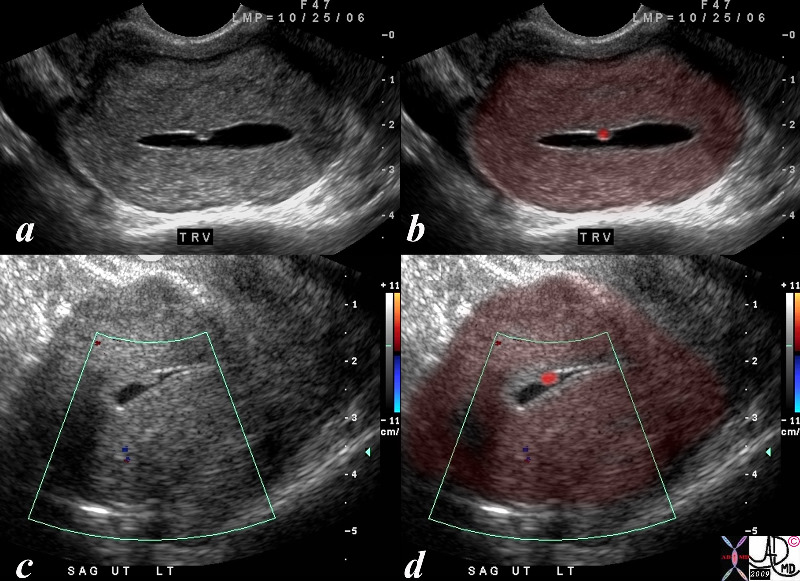
Two Lesions in the Junctional Zone Impinging on the Endometrium
|
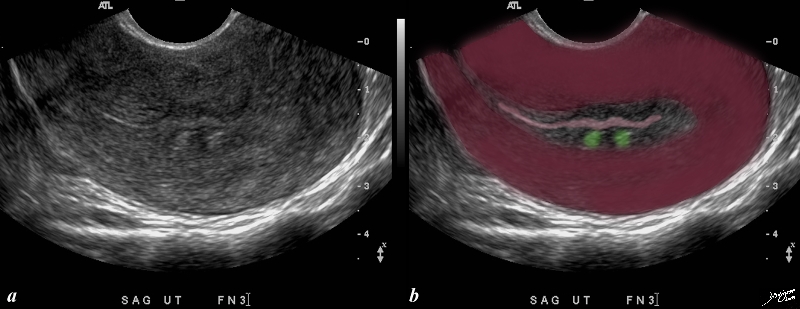
| This patient presents with menorrhagia. Two echogenic nodules (overlaid in green) are seen in the subendometrial layer, (junctional zone). They are in close proximity and do appear to have appositional relationships with the endometrial stripe. They appear to and distort the endometrial lining. These findings could account for the patient’s menorrhagia. Note that the uterus is retroverted Included in the differential diagnosis are submucosal fibroids, and dystrophic changes in prior foci of adenomyosis. An MRI would be helpful in further characterizing these lesions in the subendometrial layer
copyright 2009 all rights resrved Courtesy Ashley Davidoff MD 85641bc01.8s |
References
Casilla J Joseph R and Guerra J CT appearance of Uterine Leiomyomas Radiographics 1990 10:999-1007
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Two Lesions in the Junctional Zone Impinging on the Endometrium
This patient presents with menorrhagia. Two echogenic nodules (overlaid in green) are seen in the subendometrial layer, (junctional zone). They are in close proximity and do appear to have appositional relationships with the endometrial stripe. They appear to and distort the endometrial lining. These findings could account for the patient’s menorrhagia. Note that the uterus is retroverted Included in the differential diagnosis are submucosal fibroids, and dystrophic changes in prior foci of adenomyosis. An MRI would be helpful in further characterizing these lesions in the subendometrial layer
copyright 2009 all rights resrved Courtesy Ashley Davidoff MD 85641bc01.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Two Lesions in the Junctional Zone Impinging on the Endometrium
This patient presents with menorrhagia. Two echogenic nodules (overlaid in green) are seen in the subendometrial layer, (junctional zone). They are in close proximity and do appear to have appositional relationships with the endometrial stripe. They appear to and distort the endometrial lining. These findings could account for the patient’s menorrhagia. Note that the uterus is retroverted Included in the differential diagnosis are submucosal fibroids, and dystrophic changes in prior foci of adenomyosis. An MRI would be helpful in further characterizing these lesions in the subendometrial layer
copyright 2009 all rights resrved Courtesy Ashley Davidoff MD 85641bc01.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This patient presents with menorrhagia. Two echogenic nodules (overlaid in green) are seen in the subendometrial layer, (junctional zone). They are in close proximity and do appear to have appositional relationships with the endometrial stripe. They appear to and distort the endometrial lining. These findings could account for the patient’s menorrhagia. Note that the uterus is retroverted Included in the differential diagnosis are submucosal fibroids, and dystrophic changes in prior foci of adenomyosis. An MRI would be helpful in further characterizing these lesions in the subendometrial layer
copyright 2009 all rights resrved Courtesy Ashley Davidoff MD 85641bc01.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This patient presents with menorrhagia. Two echogenic nodules (overlaid in green) are seen in the subendometrial layer, (junctional zone). They are in close proximity and do appear to have appositional relationships with the endometrial stripe. They appear to and distort the endometrial lining. These findings could account for the patient’s menorrhagia. Note that the uterus is retroverted Included in the differential diagnosis are submucosal fibroids, and dystrophic changes in prior foci of adenomyosis. An MRI would be helpful in further characterizing these lesions in the subendometrial layer
copyright 2009 all rights resrved Courtesy Ashley Davidoff MD 85641bc01.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Two Lesions in the Junctional Zone Impinging on the Endometrium
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Two Lesions in the Junctional Zone Impinging on the Endometrium
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Prolapsing Submucosal Fibroid
This patient presented to the emergency room with severe crampy abdominal pain and a known history of a submucosal fibroid. The MRI shows the fibroid (dark pink) orotruding and expanding the cervix in the sagital view, and in the coronal view it is seen as a hyperemic structure (c) surrounded by lighter pink myometrium.
pain uterus submucosal fibroid prolapse MRI Courtesy Ashley DAvidoff MD copyright 2008 16265c01.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Prolapsing Submucosal Fibroid
This patient presented to the emergency room with severe crampy abdominal pain and a known history of a submucosal fibroid. The MRI shows the fibroid (dark pink) orotruding and expanding the cervix in the sagital view, and in the coronal view it is seen as a hyperemic structure (c) surrounded by lighter pink myometrium.
pain uterus submucosal fibroid prolapse MRI Courtesy Ashley DAvidoff MD copyright 2008 16265c01.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => This patient presented to the emergency room with severe crampy abdominal pain and a known history of a submucosal fibroid. The MRI shows the fibroid (dark pink) orotruding and expanding the cervix in the sagital view, and in the coronal view it is seen as a hyperemic structure (c) surrounded by lighter pink myometrium.
pain uterus submucosal fibroid prolapse MRI Courtesy Ashley DAvidoff MD copyright 2008 16265c01.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => This patient presented to the emergency room with severe crampy abdominal pain and a known history of a submucosal fibroid. The MRI shows the fibroid (dark pink) orotruding and expanding the cervix in the sagital view, and in the coronal view it is seen as a hyperemic structure (c) surrounded by lighter pink myometrium.
pain uterus submucosal fibroid prolapse MRI Courtesy Ashley DAvidoff MD copyright 2008 16265c01.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Prolapsing Submucosal Fibroid
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Prolapsing Submucosal Fibroid
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Submucosal Fibroid
The USscan (sonohysterogram) scan is from a 41year old female, who presents with dysfunctional uterine bleeding. The study reveals a 4mms submucosal nodule shown at pathology to be a submucosal fibroid.
uterus fibroid leiomyoma submucosal USscan sonohysterogram Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 84299c041.8
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Submucosal Fibroid
The USscan (sonohysterogram) scan is from a 41year old female, who presents with dysfunctional uterine bleeding. The study reveals a 4mms submucosal nodule shown at pathology to be a submucosal fibroid.
uterus fibroid leiomyoma submucosal USscan sonohysterogram Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 84299c041.8
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] => The USscan (sonohysterogram) scan is from a 41year old female, who presents with dysfunctional uterine bleeding. The study reveals a 4mms submucosal nodule shown at pathology to be a submucosal fibroid.
uterus fibroid leiomyoma submucosal USscan sonohysterogram Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 84299c041.8
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] => The USscan (sonohysterogram) scan is from a 41year old female, who presents with dysfunctional uterine bleeding. The study reveals a 4mms submucosal nodule shown at pathology to be a submucosal fibroid.
uterus fibroid leiomyoma submucosal USscan sonohysterogram Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 84299c041.8
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Submucosal Fibroid
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Submucosal Fibroid
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Leiomyosarcoma
The CT is from a 58 year old post menopausal female who presents with an enlarging pelvic mass (a,b,c). CTscan shows multiple large masses in the uterus some of which are calcified consistent with leiomyomas. However clinically the mass had grown significantly in the last few months. Surgery revealed a leiomyosarcoma. Follow up CT 1 year later showed paracolic nodules which were proven to be metastatic deposits by biopsy (d).
Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 85519cL.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Leiomyosarcoma
The CT is from a 58 year old post menopausal female who presents with an enlarging pelvic mass (a,b,c). CTscan shows multiple large masses in the uterus some of which are calcified consistent with leiomyomas. However clinically the mass had grown significantly in the last few months. Surgery revealed a leiomyosarcoma. Follow up CT 1 year later showed paracolic nodules which were proven to be metastatic deposits by biopsy (d).
Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 85519cL.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The CT is from a 58 year old post menopausal female who presents with an enlarging pelvic mass (a,b,c). CTscan shows multiple large masses in the uterus some of which are calcified consistent with leiomyomas. However clinically the mass had grown significantly in the last few months. Surgery revealed a leiomyosarcoma. Follow up CT 1 year later showed paracolic nodules which were proven to be metastatic deposits by biopsy (d).
Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 85519cL.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The CT is from a 58 year old post menopausal female who presents with an enlarging pelvic mass (a,b,c). CTscan shows multiple large masses in the uterus some of which are calcified consistent with leiomyomas. However clinically the mass had grown significantly in the last few months. Surgery revealed a leiomyosarcoma. Follow up CT 1 year later showed paracolic nodules which were proven to be metastatic deposits by biopsy (d).
Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 85519cL.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Leiomyosarcoma
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Leiomyosarcoma
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Benign Systemic Leiomyomatosis
This is a collage of CT findings of benign systemic leiomyomatosis over a 4 and half year period. Images 1,2,3 are from April 20th 1999 when the patient presented wth a pelvic mass with extensive hyperemic fibroid disease. Following hysterectomy a repeat CT of March 17 2000 shows residual disease in the pelvis, right internal iliac, and left internal iliac nodes (4,5,6). By November 2003 there was loss of the hyperemia and significant reduction of the tumor bulk. The patient was aged 47 at this time with a history of hepatitis being treated with interferon.
Courtesy Ashley Davidoff MD. – 32481c01
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Benign Systemic Leiomyomatosis
This is a collage of CT findings of benign systemic leiomyomatosis over a 4 and half year period. Images 1,2,3 are from April 20th 1999 when the patient presented wth a pelvic mass with extensive hyperemic fibroid disease. Following hysterectomy a repeat CT of March 17 2000 shows residual disease in the pelvis, right internal iliac, and left internal iliac nodes (4,5,6). By November 2003 there was loss of the hyperemia and significant reduction of the tumor bulk. The patient was aged 47 at this time with a history of hepatitis being treated with interferon.
Courtesy Ashley Davidoff MD. – 32481c01
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
This is a collage of CT findings of benign systemic leiomyomatosis over a 4 and half year period. Images 1,2,3 are from April 20th 1999 when the patient presented wth a pelvic mass with extensive hyperemic fibroid disease. Following hysterectomy a repeat CT of March 17 2000 shows residual disease in the pelvis, right internal iliac, and left internal iliac nodes (4,5,6). By November 2003 there was loss of the hyperemia and significant reduction of the tumor bulk. The patient was aged 47 at this time with a history of hepatitis being treated with interferon.
Courtesy Ashley Davidoff MD. – 32481c01
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
This is a collage of CT findings of benign systemic leiomyomatosis over a 4 and half year period. Images 1,2,3 are from April 20th 1999 when the patient presented wth a pelvic mass with extensive hyperemic fibroid disease. Following hysterectomy a repeat CT of March 17 2000 shows residual disease in the pelvis, right internal iliac, and left internal iliac nodes (4,5,6). By November 2003 there was loss of the hyperemia and significant reduction of the tumor bulk. The patient was aged 47 at this time with a history of hepatitis being treated with interferon.
Courtesy Ashley Davidoff MD. – 32481c01
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Benign Systemic Leiomyomatosis
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Benign Systemic Leiomyomatosis
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Large Intramural Fibroid Deforming the Stripe
T2 Weighted Image
In this sagittal view of the T2 weighted MRI of the uterus of a 46 year old female an almost 6cms slightly hyperintense fibroid is seen pushing on the endometrial cavity from above. This patient has a large fibroid aka leiomyoma that impinges on the endometrial cavity.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 96570.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Large Intramural Fibroid Deforming the Stripe
T2 Weighted Image
In this sagittal view of the T2 weighted MRI of the uterus of a 46 year old female an almost 6cms slightly hyperintense fibroid is seen pushing on the endometrial cavity from above. This patient has a large fibroid aka leiomyoma that impinges on the endometrial cavity.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 96570.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
In this sagittal view of the T2 weighted MRI of the uterus of a 46 year old female an almost 6cms slightly hyperintense fibroid is seen pushing on the endometrial cavity from above. This patient has a large fibroid aka leiomyoma that impinges on the endometrial cavity.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 96570.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
In this sagittal view of the T2 weighted MRI of the uterus of a 46 year old female an almost 6cms slightly hyperintense fibroid is seen pushing on the endometrial cavity from above. This patient has a large fibroid aka leiomyoma that impinges on the endometrial cavity.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 96570.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Large Intramural Fibroid Deforming the Stripe
T2 Weighted Image
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Large Intramural Fibroid Deforming the Stripe
T2 Weighted Image
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Deformity of the Endometrial CAvity Caused by an Intramural Fibroid
In this sagittal view of the T1 weighted contrast enhanced study of the the uterus of a 46 year old female. The uterus roughly retains its pear shaped structure but the shape of the endometrial cavity is distinctly abnormal as if there is something pushing on it from above. This patient has a diffusely enhancing isointense leiomyoma that impinges on the endometrial cavity.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 96577.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Deformity of the Endometrial CAvity Caused by an Intramural Fibroid
In this sagittal view of the T1 weighted contrast enhanced study of the the uterus of a 46 year old female. The uterus roughly retains its pear shaped structure but the shape of the endometrial cavity is distinctly abnormal as if there is something pushing on it from above. This patient has a diffusely enhancing isointense leiomyoma that impinges on the endometrial cavity.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 96577.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
In this sagittal view of the T1 weighted contrast enhanced study of the the uterus of a 46 year old female. The uterus roughly retains its pear shaped structure but the shape of the endometrial cavity is distinctly abnormal as if there is something pushing on it from above. This patient has a diffusely enhancing isointense leiomyoma that impinges on the endometrial cavity.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 96577.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
In this sagittal view of the T1 weighted contrast enhanced study of the the uterus of a 46 year old female. The uterus roughly retains its pear shaped structure but the shape of the endometrial cavity is distinctly abnormal as if there is something pushing on it from above. This patient has a diffusely enhancing isointense leiomyoma that impinges on the endometrial cavity.
Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 96577.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Deformity of the Endometrial CAvity Caused by an Intramural Fibroid
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Deformity of the Endometrial CAvity Caused by an Intramural Fibroid
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Large and Lobular Uterus
The CTscan is from a 31year old female, who presents with a pelvic mass.The study reveals a large uterus with multicentric fibroids and mild hydronephrosis The heterogeneous and lobular mass measures 17cms (c-c)by 10cms (A-P) by 12cms (transverse), and is consistent with a fibroid uterus.
Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 84362c.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Large and Lobular Uterus
The CTscan is from a 31year old female, who presents with a pelvic mass.The study reveals a large uterus with multicentric fibroids and mild hydronephrosis The heterogeneous and lobular mass measures 17cms (c-c)by 10cms (A-P) by 12cms (transverse), and is consistent with a fibroid uterus.
Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 84362c.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The CTscan is from a 31year old female, who presents with a pelvic mass.The study reveals a large uterus with multicentric fibroids and mild hydronephrosis The heterogeneous and lobular mass measures 17cms (c-c)by 10cms (A-P) by 12cms (transverse), and is consistent with a fibroid uterus.
Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 84362c.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The CTscan is from a 31year old female, who presents with a pelvic mass.The study reveals a large uterus with multicentric fibroids and mild hydronephrosis The heterogeneous and lobular mass measures 17cms (c-c)by 10cms (A-P) by 12cms (transverse), and is consistent with a fibroid uterus.
Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 84362c.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Large and Lobular Uterus
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Large and Lobular Uterus
)
