
The Common Vein Copyright 2007
POSITION OF THE PANCREAS
In this section we consider the position of the pancreas in the abdominal cavity. Its Dr Jekyll and Mr Hyde positional duality surfaces at this point since the head body and some of the tail are located within the retroperitoneum, while the distal tip of the tail is enveloped in the splenorenal ligament and thus considered intraperitoneal. There are few structures that share the duality of being both an intraperitoneal and retroperitoneal structure. These include the duodenum which has 1st portion, part of the 2nd and 4th portions within the peritoneal cavity, while part of the 2nd and all of the third are retroperitoneal. The colon shares the privilege with ascending and descending colon being retroperitoneal while the remaining portions of the colon are intraperitoneal. What makes any structure an intraperitoneal structure? – when more than 2/3rds of the organ is covered by peritoneum it is considered peritoneal.
The pancreas has been described as the hermit or hidden organ of the abdomen. It is surrounded on all 4 sides by parts of the gastrointestinal tract and has the stomach and lesser sac covering its anterior surface with the liver forming a second anterior and lateral layer. The spine aorta, IVC, splenic vein and left renal vein lie directly posterior while the kidneys lie posterior and lateral to it. On its right side is the antrum descending duodenum and right lobe of the liver with the right colon, and on its left is duodenum proximal small bowel colon and spleen. Superiorly the splenic artery and body of stomach protect the gland and inferiorly lies the transverse duodenum. The gland is so well covered that the surgeon, even with the abdomen totally opened has trouble accessing it easily.
The pancreas cannot be palpated clinically and even when the abdomen is opened, the surgeon has difficulty in seeing or even fully palpating the pancreas. In fact it was one of the few organs that eluded the magical eye of Leonardo da Vinci. Small limited views of the pancreas are only accessible through supracolic, right infracolic and the left infracolic compartments. The foramen of Winslow, also allows a limited peek feel of the neck of the pancreas. If further surgical inspection is necessary then maneuvers such as the Kocher maneuver can be utilized by incising peritoneum lateral to the second part of the duodenum or opening the lesser omentum to gain access into the lesser sac and the pancreas.
As the central organ in the upper abdomen it crosses the abdomen from the right side of the retroperitoneum where the head lies to the right of the spine at about L2 level and to the left for about 10cms in an upward course to the hilum of the spleen at the L1 . It thus is mostly leftward in its position, and covers the area known as the transpyloric plane. (L1-L2)
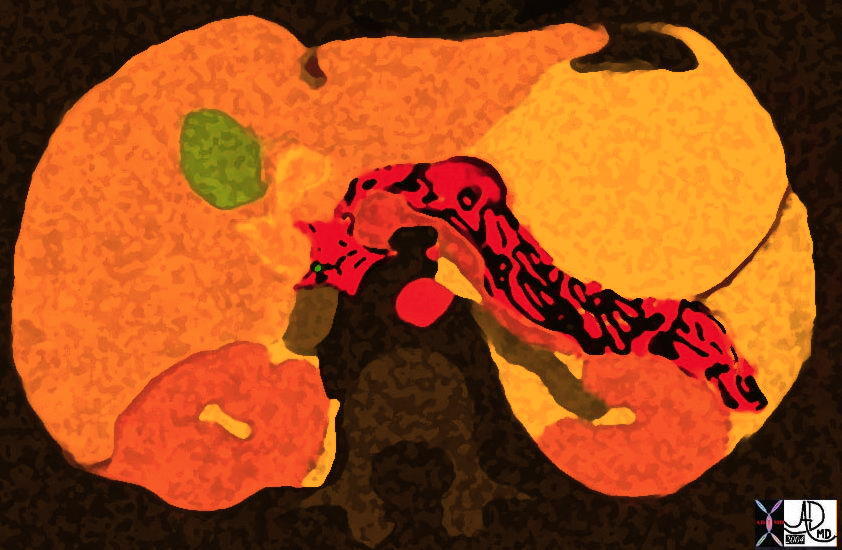 Pancreas in the Fall just before Halloween 38025b12 Courtesy Ashley Davidoff MD
Pancreas in the Fall just before Halloween 38025b12 Courtesy Ashley Davidoff MD
The retroperitoneum is divided into three major compartments – the anterior pararenal space, the perirenal space and the posterior pararenal space. The pancreas lies in the anterior pararenal space, and shares this space with the transverse duodenum, and great vessels. The latter have been given a subcompartment by some authors, called the central retroperitoneum, since the great vessels seem to be protected from anterior pararenal space disease.
Long Axis:
Its axis is therefore dominantly but not strictly transverse.
The pancreas extends from the duodenal loop to the splenic hilum diagonally across the body at about the L1 -L2 level It can be divided anatomically into a head, neck, body, and tail. 4 The neck lies anterior to the superior mesenteric vein and proximal portion of the main portal vein formed by the confluence of the superior mesenteric and splenic veins. The head of the pancreas lies lateral to the neck, nestled in the C-loop of the duodenum. In this area it lies anterior to the inferior vena cava and right crus of the diaphragm. The inferomedial portion of the head is called the uncinate process, which varies greatly in size. It lies posterior to the superior mesenteric vein and, in about 5c% of patients, it lies posterior to the proximal superior mesenteric artery. The body of the pancreas lies anterior to the abdominal aorta below the origin of the celiac axis and anterior to the origin of the superior mesenteric artery. The tail is anterior to the left crus of the diaphragm, the left adrenal gland, and the left kidney, from which it is separated by the anterior portion of Gerota’s fascia
Position – surface anatomy
The neck of the pancreas lies in the transpyloric plane in the midline. The body can be imagined passing obliquely upwards and to the left for about 10 cm and the head downwards and to the right to lie in the curve of duodenum.
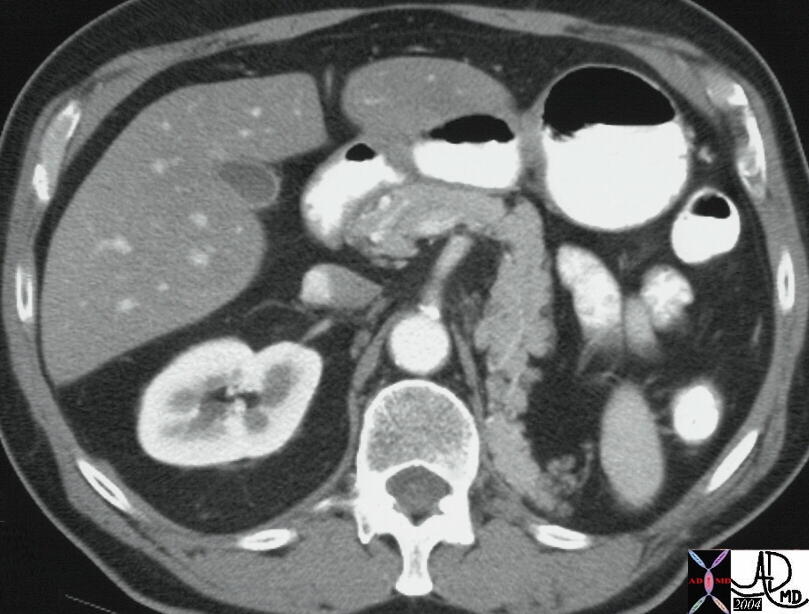
 This CT scan demonstrates the abnormal mirror image position of the pancreas in a patient wiith situs inversus. Note the left sided position of the IVC and liver. 28007b02 Courtesy Ashley Davidoff MD
This CT scan demonstrates the abnormal mirror image position of the pancreas in a patient wiith situs inversus. Note the left sided position of the IVC and liver. 28007b02 Courtesy Ashley Davidoff MD
 This CT scan demonstrates the abnormal mirror image position of the pancreas in a patient wiith situs inversus. 28008 Courtesy Ashley DAvidoff MD.
This CT scan demonstrates the abnormal mirror image position of the pancreas in a patient wiith situs inversus. 28008 Courtesy Ashley DAvidoff MD.
Position – application to disease
The relationship of the pancreatic neck to the spine renders it vulnerable in trauma.
A Chance fracture is an horizontal fracture thru vertebra (body, pedicles, laminae)
caused by sudden deceleration with lap-only seatbelt usually involving L1 or L2, and usually involving children.
Associated intra-abdominal injuries appear to be more common in the pediatric age group with incidence approaching 50%.
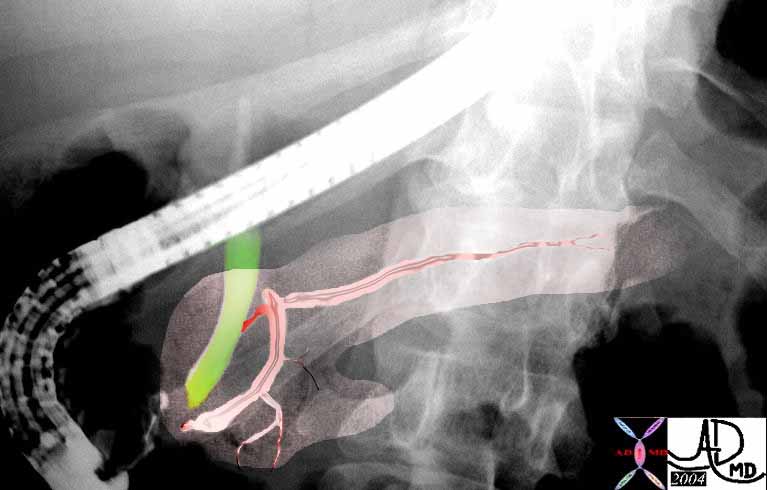 This ERCP with overlay, the relative positioning of the duct in relation to the pancreas and the bile duct., but also its position in relation to the spine. It is easy to envisahe how the Chance fracture of the spine can affect the pancreas. Note also the bifid appearance to the duct in the tail which is a normal and common variant. Courtsy Ashley DAvidoff MD. 39962b04
This ERCP with overlay, the relative positioning of the duct in relation to the pancreas and the bile duct., but also its position in relation to the spine. It is easy to envisahe how the Chance fracture of the spine can affect the pancreas. Note also the bifid appearance to the duct in the tail which is a normal and common variant. Courtsy Ashley DAvidoff MD. 39962b04
Islets of Langerhans
Surprisingly the islets of Langerhans represent only 1-2% of the volume of the pancreas. They are most numerous in the tail.
The central position of the pancreas in the abdomen creates many alternate routes for its lymphatic drainage. In health this is a good thing, but in disease, and specifically in malignant disease, there are a wide variety of routes for spread and thus disease may extend over a large regional area, including the splenic, hepatic, and superior mesenteric nodal systems as well as the aortocaval and other posterior abdominal wall lymphatics.
Additionally the pancreas is so intimate with major vascular structures. Most important is its grasp and intimate contact with the SMV-portal confluence, and SMA in the fold of the uncinate process. The celiac axis, with its major branches – hepatic splenic and gastroduodenal arteries all abut the gland. The splenic vein lies posteriorly and frequently is involved in both inflammatory and neoplastic processes. The aorta which lies posterior to the pancreas is usually spared of spread of pancreatic disease, though the lower pressure IVC may be compressed and become thrombosed by diseases in the pancreatic head. Because all the important vessels are packed so close together, a short distance of tumor spread to the superior mesenteric vein, will involve the portal vein, and involvement of either usually renders the patient incurable.
 This CT scan through the pancreas shows a pancreas with the shape of a “7” caused by a displacement of the body and tail of the pancreas into the left renal bed. This has been caused by a nephrectomy and seondary “filling in ” of the empty space. 25196 Courtesy Ashley Davidoff MD
This CT scan through the pancreas shows a pancreas with the shape of a “7” caused by a displacement of the body and tail of the pancreas into the left renal bed. This has been caused by a nephrectomy and seondary “filling in ” of the empty space. 25196 Courtesy Ashley Davidoff MD
Accessory pancreas
“the part of the head lying behind the mesenteric vessels may be separate from the remainder of the gland, forming what is called the lesser (accessory) pancreas.
Various examples of an accessory pancreas have been described after the initial description by Klob in 1859. They may occur in the mesentery of the small intestine, the wall of the duodenum, the upper part of the jejunum, or more rarely, in the wall of the stomach, ileum, gallbladder, or spleen. They are generally situated either in the submucosa or the subserous coat, but may extend into the muscular layer. An accessory pancreas was found near the origin of the inferior mesenteric artery in an 11-year old boy. The size of these masses varies in diameter, from a few millimeters to 5cm and their own ducts. The masses may contain pancreatic islet cells. In a few cases, some pancreatic tissue has been found at the blind end of intestinal (Meckel’s) diverticula. They may appear in any derivative of the foregut, from stomach to the ileal (Meckel’s) diverticulum including the spleen and gallbladder, but not the large intestine. They are most common in the duodenum.”
Position – application to imaging
As a retroperitoneal organ behind the stomach and framed by gas filled small and large bowel, the pancreas sometimes is suboptimally visualised by ultrasound. This is particularly true in diseases such as pancreatitis when small bowel ileus results in gas filled bowel, resulting in an obstructed view of the pancreas. Filling the stomach with water sometimes does aid in the examination by acting to improve ultrasound transmission. The tail hidden in the hilum can sometimes be only visualised by using the sppleen as a window.
CT is far better suited to to provide consistent imaging of the retroperitoneum. It easily can circumvent the problems discussed with ultrasound transmission. The MDCT technology has allowed exquisite detail to be portrayed by CT, and it promises only to improve in the future. The presence of disease is sometimes only suggested by subtle thickening of Gerota’s fascia or the lateral conal fascia – detail that can only be portrayed by CT. For the retropewritoneum – MDCT is the king and the queen
CHARACTER OR NATURE OF THE PANCREAS
In this section we discuss the macroscopic nature of the gland in health and disease. We explore the way the gland looks and feels and the way it reacts to an interrogating force, such as ultrasound waves, X-rays, and proton manipulation by radiofrequency waves and altering magnetic gradients.
Microscopically the gland has a structure very similar to the salivary glands, but macroscopically it is far softer than the salivary glands. It is a soft, lobulated, grayish-pink gland with cauliflower-like texture. Its surface is pale yellow-tan, finely nodular, and firm to palpation.
RELATIONS
The pancreas is not short on friends and neighbours. It seems to be the centre of the upper abdominal cavity and protected as the hermit from exposure for so many years by thre surrounding structures. Overall the most important and relevant relations of the pancreas are to the stomach, duodenum, and mesenteries.
 This acquatic scene shows th relationship of the pancreas to its neighbours particulalrly the splenic vein and left renal vein which run a parallel course, almost like a bunch of buddies romping in the water. The SMA lies under the splenic vein-portal vein confluence as it courses at 90 degrees to the course of the other structures. 24796b07 Courtesy Ashley Davidoff MD
This acquatic scene shows th relationship of the pancreas to its neighbours particulalrly the splenic vein and left renal vein which run a parallel course, almost like a bunch of buddies romping in the water. The SMA lies under the splenic vein-portal vein confluence as it courses at 90 degrees to the course of the other structures. 24796b07 Courtesy Ashley Davidoff MD
Relations of the Head of the Pancreas
The head of the pancreas is located within the curve of the duodenum and is embraced by it. It has a prolongation, called the uncinate process (L. hook-shaped). This extends superiorly and to the left and lies posterior to the superior mesenteric vessels. Here, it rests against the aorta posteriorly. The head rests posteriorly on the IVC as well as the right renal vessels, and the left renal vein.
The bile duct, on its way to the duodenum, lies in a groove on the posterosuperior surface of the head of the pancreas; sometimes it is embedded in it.
The anterior relations include the GDA, and the transverse colon. The posterior relations include the confluens of the SMV and splenic veins to form the portal vein, inferior vena cava, right crus of diaphragm, aorta, and bile duct.
Relations of the Neck of the Pancreas
It is about 2 cm long, is continuous with the head and merges imperceptibly into the body of the pancreas. The neck is grooved posteriorly by the superior mesenteric vessels. Its anterior surface is covered with peritoneum and is adjacent to the pylorus of the stomach. The superior mesenteric vein joins the splenic vein to form the portal vein posterior to the neck of the pancreas. Anterior relations include the GDA, pylorus, and part of the omental bursa. The posterior relations include the SMV and beginning of portal vein.
Relations of the Body of the Pancreas
The anterior relations of the body of the pancreas include the posterior layer of the peritoneum while the posterior relations include the aorta, origin of SMA, left crus of the diaphragm, left adrenal, left kidney, left renal vessels, and particularly the left renal vein, and splenic vein. Inferiorly the peritoneum, transverse mesocolon, duodenojejunal flexure, jejunum, left colic flexure form neighbours while superiorly the splenic artery, celiac axis, common hepatic artery reside. Anteriorly there is the transverse mesocolon .
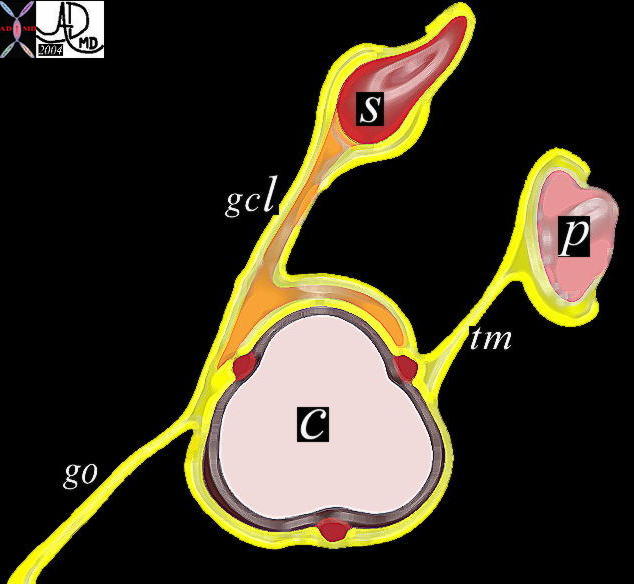 This is a very important diagram which is used repeatedly to define the omental and ligamentous relationships between the pacreas colon and stomach. It also shos the position of the pancreas in the retroperitoneum. The posterior peritoneum (yellow) lies partially surrounding the anterior portion of the pancreas and gives rise to the transverse mesocolon which forms a ligamentous attachment as a double layer to the transverse colon. Disease o the pancreas can thus reach the colon by this route. 01443b05 Courtesy Ashley Davidoff MD P = pancreas c= transverse colon S = stomach gcl = gastrocolic ligament go = greater omentum tm = transverse mesocolon 01443b05 Courtesy Ashley Davidoff MD P = pancreas c= transverse colon S = stomach gcl = gastrocolic ligament go = greater omentum tm = transverse mesocolon
This is a very important diagram which is used repeatedly to define the omental and ligamentous relationships between the pacreas colon and stomach. It also shos the position of the pancreas in the retroperitoneum. The posterior peritoneum (yellow) lies partially surrounding the anterior portion of the pancreas and gives rise to the transverse mesocolon which forms a ligamentous attachment as a double layer to the transverse colon. Disease o the pancreas can thus reach the colon by this route. 01443b05 Courtesy Ashley Davidoff MD P = pancreas c= transverse colon S = stomach gcl = gastrocolic ligament go = greater omentum tm = transverse mesocolon 01443b05 Courtesy Ashley Davidoff MD P = pancreas c= transverse colon S = stomach gcl = gastrocolic ligament go = greater omentum tm = transverse mesocolon
The body is somewhat triangular or irregularly prismatic in shape. In cross section it has an anterior, posterior, and inferior surface. The anterior surface is covered with peritoneum and forms part of the bed of the stomach. This anterior surface provides attachment for the transverse mesocolon. Peritoneum is absent from the posterior surface which is in contact with the aorta, superior mesenteric artery, left adrenal gland, and the left kidney.
The body of the pancreas is intimately related to the splenic vein. This is an important landmark for pancreatic identification particulalrly on US. The body has a small prominence, the omental tuberosity, (tuber omentale) arising from its superior border, and contacting the lesser omentum This tuberosity is located immediately inferior to the celiac trunk