Alok Anand MD
The Common Vein Copyright 2010
Introduction
CT evaluation of the prostate is rarely focused on the organ itself. As there is little difference in attenuation between the various zones, it usually appears fairly homogeneous without distinction between laysers.. In the setting of infection or abscess, inhomogeneities may become apparent. In addition, lymphadenopathy is easily seen.
CT scan is the a radiological study that uses X-ray technology combined with computer technology to visualize the structures of the body. In general for abdominal imaging, it provides a global view of all the abdominal structures, providing excellent results in almost all patients since there is little operator dependance. Intravenous contrast is utilized, although oral contrast may be used if evaluating the neighboring bowels, and the current multidetector technology enables the whole abdomen to be scanned in 10-15 seconds. With respect to the prostate no specific protocols are used and the intent of using CT is to visualize structures related to the prostate disease, and not necessarily the prostate itself, which is best visualized by transrectal ultrasound.
Principles
Computed tomography is an imaging technique where X-ray technology and computer technology are used to produce transverse or axial tomograms of the body. X-ray generators and detectors are positioned in a doughnut type ring around the body. The X-ray generators produce highly collimated X-ray beams which interact with the tissue from many different angles and the result is detected and recorded by the detectors that are aligned in a ring oppposite the generators. Each tissue has specific attenuation characteristics. The attenuation of the x-rays of a specific tissue obtained from multiple projections is collected by a computer which organizes and displays the information using mathematical algorithms.
Indications
CT provides a global view of the abdomen/pelvis and is indicated as secondary study for most prostate disease particularly when complications are suspected. In prostatitis, CT enables visualization of neighboring structures for fluid or abscess collections. PET CT is of limited use in evaluating prostate cancer, as it rarely demonstrates adequate hypermetabolic activity to be seen. Nevertheless, contrast-enhanced multidetector CT is useful in evaluating lymphadenopathy and distant spread of disease, most often lytic bone disease, in addition ot liver and lung metastases.
Contraindications
There is no absolute contraindication to utuilizing CT since it its benefits almost always outweigh the risks. CT should also not be used in young men if ultrasound has potential application. Contrast studies should be exercised with caution in the patient populations mentioned above, as well as in patients with renal insufficiency, as iodinated contrast can cause further damage to renal parenchyma, possibly resulting in acute kidney injury requiring dialysis, or even death.
Advantages
CT imaging offers a global view of the abdomen. With one or two sequences it allows us to see the organs, bladder and genitourinary tract, small calcifications, peritoneal fat and mesenteries, blood vessels and the bones mostly with exquisite detail. CT can be used to image both soft-tissue and bony tissue. CT can be used during interventional procedures, allowing percutaneous drainage, biopsy or ostomy placement,avoiding more invasive therapies.
Disadvantages
In addition to exposing patients to potentially harmful ionizing radiation it carries risk of radiation exposure to healthcare personnel as well. As such, its use should be accompanied by appropriate safety precautions, such as adequate shielding and the use of failsafe techniques. Personnel should also be monitored regularly for cumulative exposure to ionizing radiation. CT does not differentiate the zonal anatomy of the prostate, paticularly without the use of contrast. For this, MRI and Ultrasound provide greater detail.
Aim
The purpose of using CT scan is usually when disease other than prostate is suspected. In the setting of external beam radiation therapy, CT is useful for treatment planning.
Method
Patient Preparation
There is no fasting requirement. Intravenous contrast may be utilized.
Equipment
No additional equipment is required for CT imaging of the prostate.
Technique
Typically pelvic imaging is done with a fasting patient in supine position. In the case of treatment planning for radiation therapy, the patient may be in the prone position. The patient then passes through the gantry, as the source spins around it, passing x-rays through at multiple angles, to be detected by sensors within the gantry and sent to a computer for processing and reconstruction. Once generated, these images may be further processed to reconstruct images in slices along other planes, such as coronal, sagital, or oblique.
Result
Although CT is not often used as a primary modality for evaluation of the prostate, CT images of the pelvis can provide some information about the prostate.
Landmarks in imaging
The prostate is normally seen at the base of the bladder. It usually appreas as a homogeneous body of soft tissue, measuring upwards of 4cm in greatest diameter. Paired seminal vessicles create a characteristic bow-tie like appearing soft tissue between the bladder and the prostate. A plane of fat separates the prostate laterally from the obturator internus muscle.
Normal
|
Normal Size Prostate 26 Year Old Male |
|
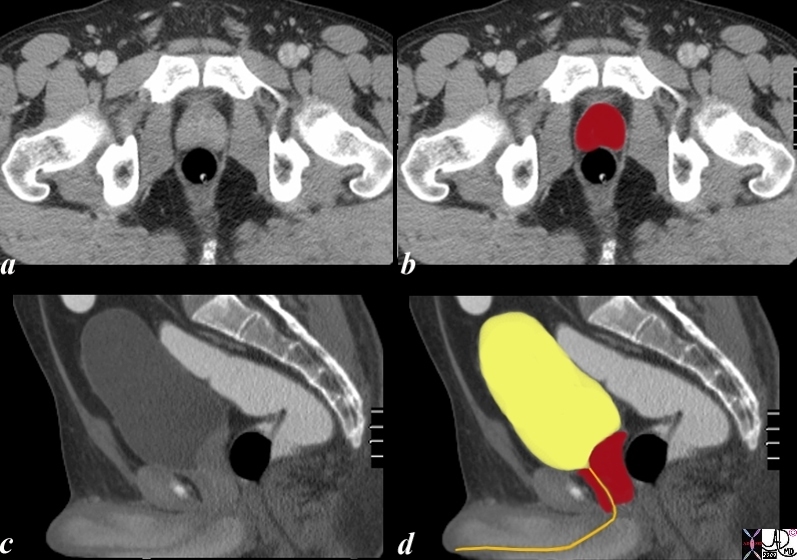
The CTscan is from a 26 year old male with a normal prostate seen in the axial plane (a,b) and in the sagittal planes (c,d). The bladder is distended. Note the shape of the gland in the transverse planer is heart shaped and in the sagittal plane almost rectangular when normal in size. The internal sphincter surrounds the top of the urethra at the base of the bladder and the urethra extends through the prostate as the prostatic urethra and into the penile urethra.
Image Courtesy Ashley Davidoff MD Copyright 2010 99331c02.8s
|
Examples of Disease
Lymphadenopathy is readily seen, even in unenhanced CT images. Carcinoma, however is difficult to distinguish from benign hyperplasia. In approximately half of cancers, contrast enhancement may be noted focally in the peripheral zone in the setting of tumor.
Overall enlargement may be noted in carcinoma, as well as hypertrophy. In carcinoma, the contours appeare more irregular and lobulated, with visible nodules of varying density. Coarse calcifications may also be present. Cystic degeneration can also be seen.
Bladder wall thickening and trabeculations are also comon stigmata of obstruction at the level of the prostate.
The aging prostate may demonstrate calcifications. An enlarged prostate may also be a risk factor for urolithiasis or stones in the urinary tract.
Abscess
Prostate Abscess |
|
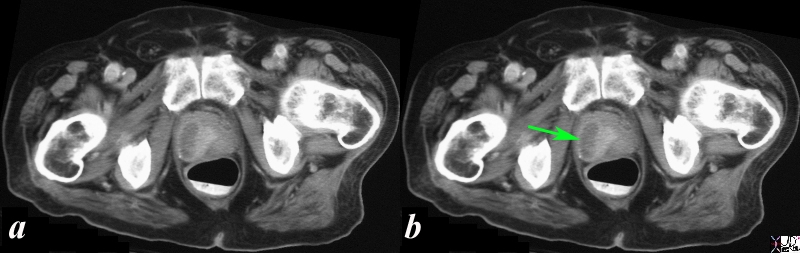
The CT scan of the pelvis is from a 63 year old man with a history of fever and pain. A fluid containing ovoid structure (green arrow b) in the prostate is surrounded by a region of hyperemia. These findings are consistent with the diagnosis of a prostatic abscess.
Image Courtesy Ashley Davidoff MD Copyright 2010 24863c.8s
|
BPH
BPH and Visualization of the Canoe Shaped Peripheral Zone |
|
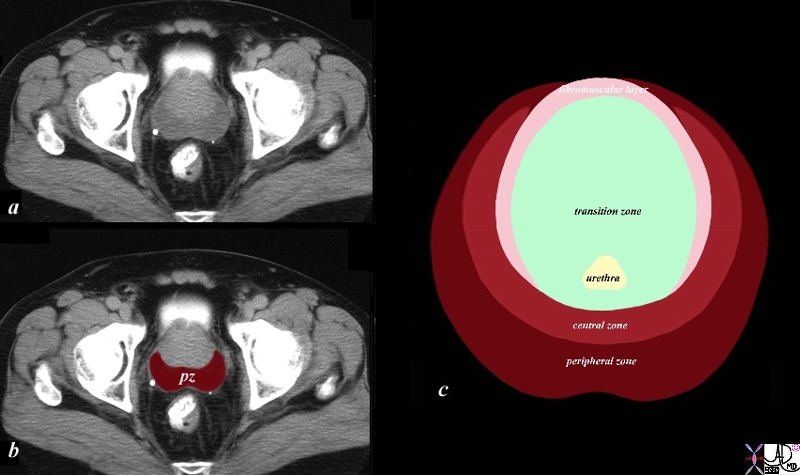
The 70 year old male shows an enlarged prostate 7.2cms in A-P by 6.1cms. in the axial plane. The gland is enlarged based on these measurements. Two distinct zones are identified. . The posterior zone is canoe shaped is hypodense and represents the peripheral zone. The anterior more hyperdense layer is combination of zones. Since the prostate gland has 4 major zones and we have accounted for the peripheral zone (pz), three other zones are present. Inward of the peripheral zone is the central zone followed by the transitional zone and finally the anterior fibromuscular layer In this patient who has benign prostatic hypertrophy (BPH) the transitional zone is enlarged due to hyperplasia. Note that BPH is a misnomer because the enlargement is due to hyperplasia and not hypertrophy. Image (c) illustrates the enlarged transitional zone which is where the hyperplasia of BPH takes place.
Image Courtesy Ashley Davidoff MD Copyright 2010 25078c04bL01.8s
|
|
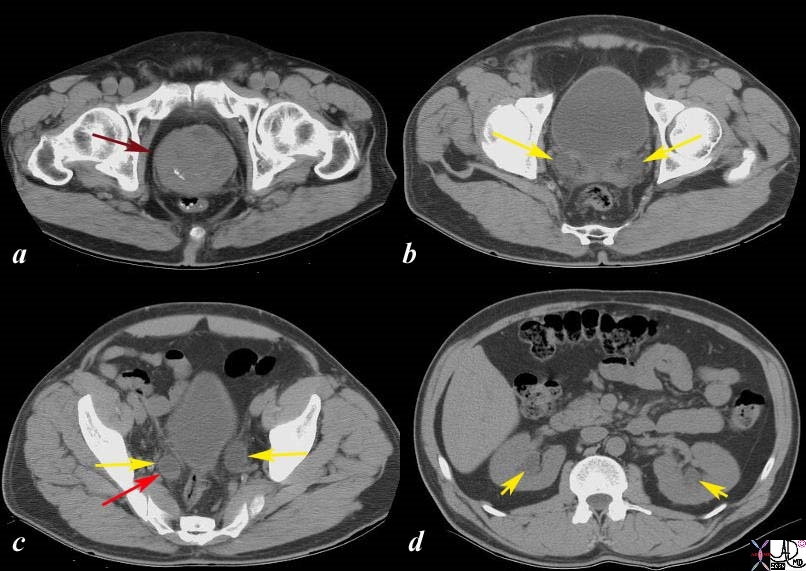
Acute Retention and Renal Obstruction |
|
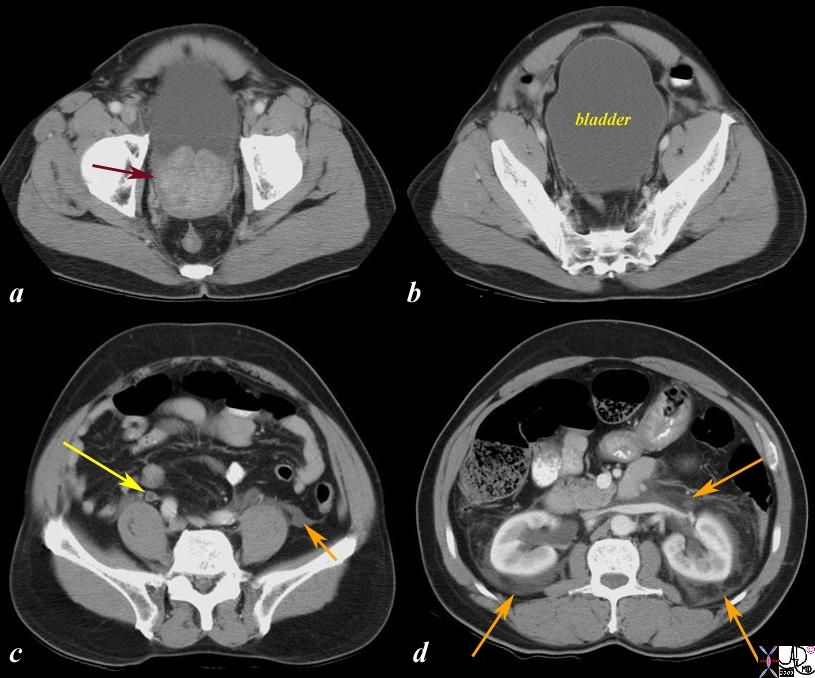
The CT scans show an enlarged prostate (a) with an enlarged bladder (b) hydroureter (c, yellow arrow) and extravasated urine (orange arrow c and d) with hydronephrosis These findings are consistent with acute obstruction of the kidneys and bladder as a result of prostatic enlargement.
Image Courtesy Ashley Davidoff MD Copyright 2010 17069c.8s
|
Carcinoma
|
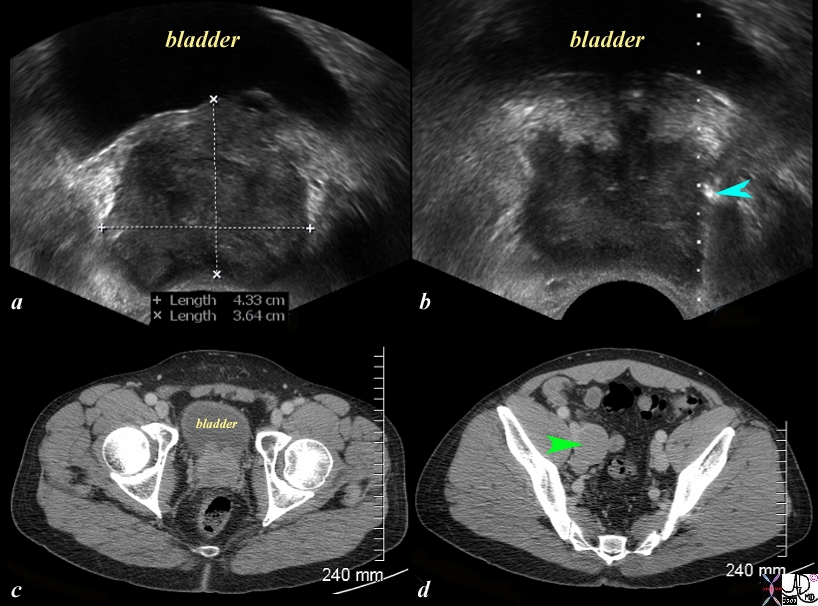
Strength and Weakness of CT scan |
|
The series of US and CTscans are from a 50 year old man with an elevated PSA Image a is a transverse ultrasound showing a minimally prominent nodular prostate. Image b shows the needle tip (teal blue arrow) in the left peripheral zone. Image c is a transverse image of the prostate showing a nodular anterior surface while image d shows an almost 3cms external iliac node. The biopsy was positive for prostate carcinoma.
Whereas ultrasound is able to characterize the lesion and provide guidance for biopsy, it is unable to consistently visualise lymph nodes and hence CT is necessary for staging. The combination of the two modalities is required. PET CT is even more helpful.
Image Courtesy Ashley Davidoff MD Copyright 2010 97374c.81s
|
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] =>
[nodeName] => table
[nodeValue] =>
Strength and Weakness of CT scan
The series of US and CTscans are from a 50 year old man with an elevated PSA Image a is a transverse ultrasound showing a minimally prominent nodular prostate. Image b shows the needle tip (teal blue arrow) in the left peripheral zone. Image c is a transverse image of the prostate showing a nodular anterior surface while image d shows an almost 3cms external iliac node. The biopsy was positive for prostate carcinoma.
Whereas ultrasound is able to characterize the lesion and provide guidance for biopsy, it is unable to consistently visualise lymph nodes and hence CT is necessary for staging. The combination of the two modalities is required. PET CT is even more helpful.
Image Courtesy Ashley Davidoff MD Copyright 2010 97374c.81s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Strength and Weakness of CT scan
The series of US and CTscans are from a 50 year old man with an elevated PSA Image a is a transverse ultrasound showing a minimally prominent nodular prostate. Image b shows the needle tip (teal blue arrow) in the left peripheral zone. Image c is a transverse image of the prostate showing a nodular anterior surface while image d shows an almost 3cms external iliac node. The biopsy was positive for prostate carcinoma.
Whereas ultrasound is able to characterize the lesion and provide guidance for biopsy, it is unable to consistently visualise lymph nodes and hence CT is necessary for staging. The combination of the two modalities is required. PET CT is even more helpful.
Image Courtesy Ashley Davidoff MD Copyright 2010 97374c.81s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 3
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The series of US and CTscans are from a 50 year old man with an elevated PSA Image a is a transverse ultrasound showing a minimally prominent nodular prostate. Image b shows the needle tip (teal blue arrow) in the left peripheral zone. Image c is a transverse image of the prostate showing a nodular anterior surface while image d shows an almost 3cms external iliac node. The biopsy was positive for prostate carcinoma.
Whereas ultrasound is able to characterize the lesion and provide guidance for biopsy, it is unable to consistently visualise lymph nodes and hence CT is necessary for staging. The combination of the two modalities is required. PET CT is even more helpful.
Image Courtesy Ashley Davidoff MD Copyright 2010 97374c.81s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The series of US and CTscans are from a 50 year old man with an elevated PSA Image a is a transverse ultrasound showing a minimally prominent nodular prostate. Image b shows the needle tip (teal blue arrow) in the left peripheral zone. Image c is a transverse image of the prostate showing a nodular anterior surface while image d shows an almost 3cms external iliac node. The biopsy was positive for prostate carcinoma.
Whereas ultrasound is able to characterize the lesion and provide guidance for biopsy, it is unable to consistently visualise lymph nodes and hence CT is necessary for staging. The combination of the two modalities is required. PET CT is even more helpful.
Image Courtesy Ashley Davidoff MD Copyright 2010 97374c.81s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Strength and Weakness of CT scan
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Strength and Weakness of CT scan
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Acute Retention and Renal Obstruction
The CT scans show an enlarged prostate (a) with an enlarged bladder (b) hydroureter (c, yellow arrow) and extravasated urine (orange arrow c and d) with hydronephrosis These findings are consistent with acute obstruction of the kidneys and bladder as a result of prostatic enlargement.
Image Courtesy Ashley Davidoff MD Copyright 2010 17069c.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Acute Retention and Renal Obstruction
The CT scans show an enlarged prostate (a) with an enlarged bladder (b) hydroureter (c, yellow arrow) and extravasated urine (orange arrow c and d) with hydronephrosis These findings are consistent with acute obstruction of the kidneys and bladder as a result of prostatic enlargement.
Image Courtesy Ashley Davidoff MD Copyright 2010 17069c.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The CT scans show an enlarged prostate (a) with an enlarged bladder (b) hydroureter (c, yellow arrow) and extravasated urine (orange arrow c and d) with hydronephrosis These findings are consistent with acute obstruction of the kidneys and bladder as a result of prostatic enlargement.
Image Courtesy Ashley Davidoff MD Copyright 2010 17069c.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The CT scans show an enlarged prostate (a) with an enlarged bladder (b) hydroureter (c, yellow arrow) and extravasated urine (orange arrow c and d) with hydronephrosis These findings are consistent with acute obstruction of the kidneys and bladder as a result of prostatic enlargement.
Image Courtesy Ashley Davidoff MD Copyright 2010 17069c.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Acute Retention and Renal Obstruction
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Acute Retention and Renal Obstruction
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
BPH and Visualization of the Canoe Shaped Peripheral Zone
The 70 year old male shows an enlarged prostate 7.2cms in A-P by 6.1cms. in the axial plane. The gland is enlarged based on these measurements. Two distinct zones are identified. . The posterior zone is canoe shaped is hypodense and represents the peripheral zone. The anterior more hyperdense layer is combination of zones. Since the prostate gland has 4 major zones and we have accounted for the peripheral zone (pz), three other zones are present. Inward of the peripheral zone is the central zone followed by the transitional zone and finally the anterior fibromuscular layer In this patient who has benign prostatic hypertrophy (BPH) the transitional zone is enlarged due to hyperplasia. Note that BPH is a misnomer because the enlargement is due to hyperplasia and not hypertrophy. Image (c) illustrates the enlarged transitional zone which is where the hyperplasia of BPH takes place.
Image Courtesy Ashley Davidoff MD Copyright 2010 25078c04bL01.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
BPH and Visualization of the Canoe Shaped Peripheral Zone
The 70 year old male shows an enlarged prostate 7.2cms in A-P by 6.1cms. in the axial plane. The gland is enlarged based on these measurements. Two distinct zones are identified. . The posterior zone is canoe shaped is hypodense and represents the peripheral zone. The anterior more hyperdense layer is combination of zones. Since the prostate gland has 4 major zones and we have accounted for the peripheral zone (pz), three other zones are present. Inward of the peripheral zone is the central zone followed by the transitional zone and finally the anterior fibromuscular layer In this patient who has benign prostatic hypertrophy (BPH) the transitional zone is enlarged due to hyperplasia. Note that BPH is a misnomer because the enlargement is due to hyperplasia and not hypertrophy. Image (c) illustrates the enlarged transitional zone which is where the hyperplasia of BPH takes place.
Image Courtesy Ashley Davidoff MD Copyright 2010 25078c04bL01.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The 70 year old male shows an enlarged prostate 7.2cms in A-P by 6.1cms. in the axial plane. The gland is enlarged based on these measurements. Two distinct zones are identified. . The posterior zone is canoe shaped is hypodense and represents the peripheral zone. The anterior more hyperdense layer is combination of zones. Since the prostate gland has 4 major zones and we have accounted for the peripheral zone (pz), three other zones are present. Inward of the peripheral zone is the central zone followed by the transitional zone and finally the anterior fibromuscular layer In this patient who has benign prostatic hypertrophy (BPH) the transitional zone is enlarged due to hyperplasia. Note that BPH is a misnomer because the enlargement is due to hyperplasia and not hypertrophy. Image (c) illustrates the enlarged transitional zone which is where the hyperplasia of BPH takes place.
Image Courtesy Ashley Davidoff MD Copyright 2010 25078c04bL01.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The 70 year old male shows an enlarged prostate 7.2cms in A-P by 6.1cms. in the axial plane. The gland is enlarged based on these measurements. Two distinct zones are identified. . The posterior zone is canoe shaped is hypodense and represents the peripheral zone. The anterior more hyperdense layer is combination of zones. Since the prostate gland has 4 major zones and we have accounted for the peripheral zone (pz), three other zones are present. Inward of the peripheral zone is the central zone followed by the transitional zone and finally the anterior fibromuscular layer In this patient who has benign prostatic hypertrophy (BPH) the transitional zone is enlarged due to hyperplasia. Note that BPH is a misnomer because the enlargement is due to hyperplasia and not hypertrophy. Image (c) illustrates the enlarged transitional zone which is where the hyperplasia of BPH takes place.
Image Courtesy Ashley Davidoff MD Copyright 2010 25078c04bL01.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
BPH and Visualization of the Canoe Shaped Peripheral Zone
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
BPH and Visualization of the Canoe Shaped Peripheral Zone
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Prostate Abscess
The CT scan of the pelvis is from a 63 year old man with a history of fever and pain. A fluid containing ovoid structure (green arrow b) in the prostate is surrounded by a region of hyperemia. These findings are consistent with the diagnosis of a prostatic abscess.
Image Courtesy Ashley Davidoff MD Copyright 2010 24863c.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Prostate Abscess
The CT scan of the pelvis is from a 63 year old man with a history of fever and pain. A fluid containing ovoid structure (green arrow b) in the prostate is surrounded by a region of hyperemia. These findings are consistent with the diagnosis of a prostatic abscess.
Image Courtesy Ashley Davidoff MD Copyright 2010 24863c.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The CT scan of the pelvis is from a 63 year old man with a history of fever and pain. A fluid containing ovoid structure (green arrow b) in the prostate is surrounded by a region of hyperemia. These findings are consistent with the diagnosis of a prostatic abscess.
Image Courtesy Ashley Davidoff MD Copyright 2010 24863c.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The CT scan of the pelvis is from a 63 year old man with a history of fever and pain. A fluid containing ovoid structure (green arrow b) in the prostate is surrounded by a region of hyperemia. These findings are consistent with the diagnosis of a prostatic abscess.
Image Courtesy Ashley Davidoff MD Copyright 2010 24863c.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Prostate Abscess
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Prostate Abscess
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => table
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 1
[previousElementSibling] => (object value omitted)
[nextElementSibling] => (object value omitted)
[nodeName] => table
[nodeValue] =>
Normal Size Prostate 26 Year Old Male
The CTscan is from a 26 year old male with a normal prostate seen in the axial plane (a,b) and in the sagittal planes (c,d). The bladder is distended. Note the shape of the gland in the transverse planer is heart shaped and in the sagittal plane almost rectangular when normal in size. The internal sphincter surrounds the top of the urethra at the base of the bladder and the urethra extends through the prostate as the prostatic urethra and into the penile urethra.
Image Courtesy Ashley Davidoff MD Copyright 2010 99331c02.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => table
[baseURI] =>
[textContent] =>
Normal Size Prostate 26 Year Old Male
The CTscan is from a 26 year old male with a normal prostate seen in the axial plane (a,b) and in the sagittal planes (c,d). The bladder is distended. Note the shape of the gland in the transverse planer is heart shaped and in the sagittal plane almost rectangular when normal in size. The internal sphincter surrounds the top of the urethra at the base of the bladder and the urethra extends through the prostate as the prostatic urethra and into the penile urethra.
Image Courtesy Ashley Davidoff MD Copyright 2010 99331c02.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
The CTscan is from a 26 year old male with a normal prostate seen in the axial plane (a,b) and in the sagittal planes (c,d). The bladder is distended. Note the shape of the gland in the transverse planer is heart shaped and in the sagittal plane almost rectangular when normal in size. The internal sphincter surrounds the top of the urethra at the base of the bladder and the urethra extends through the prostate as the prostatic urethra and into the penile urethra.
Image Courtesy Ashley Davidoff MD Copyright 2010 99331c02.8s
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
The CTscan is from a 26 year old male with a normal prostate seen in the axial plane (a,b) and in the sagittal planes (c,d). The bladder is distended. Note the shape of the gland in the transverse planer is heart shaped and in the sagittal plane almost rectangular when normal in size. The internal sphincter surrounds the top of the urethra at the base of the bladder and the urethra extends through the prostate as the prostatic urethra and into the penile urethra.
Image Courtesy Ashley Davidoff MD Copyright 2010 99331c02.8s
)
DOMElement Object
(
[schemaTypeInfo] =>
[tagName] => td
[firstElementChild] => (object value omitted)
[lastElementChild] => (object value omitted)
[childElementCount] => 2
[previousElementSibling] =>
[nextElementSibling] =>
[nodeName] => td
[nodeValue] =>
Normal Size Prostate 26 Year Old Male
[nodeType] => 1
[parentNode] => (object value omitted)
[childNodes] => (object value omitted)
[firstChild] => (object value omitted)
[lastChild] => (object value omitted)
[previousSibling] => (object value omitted)
[nextSibling] => (object value omitted)
[attributes] => (object value omitted)
[ownerDocument] => (object value omitted)
[namespaceURI] =>
[prefix] =>
[localName] => td
[baseURI] =>
[textContent] =>
Normal Size Prostate 26 Year Old Male
)
